

The Impact of Demographic, Clinical, Symptom and Psychological Characteristics on the Trajectories of Acute Postoperative Pain After Total Knee Arthroplasty
- PMID: 27165969
- PMCID: PMC5283700
- DOI: 10.1093/pm/pnw080
The Impact of Demographic, Clinical, Symptom and Psychological Characteristics on the Trajectories of Acute Postoperative Pain After Total Knee Arthroplasty
Abstract
Objective: Total knee arthroplasty is a painful procedure. No studies have evaluated modifiable predictors of acute postoperative pain trajectories during hospitalization.
Methods: Consecutive patients (N = 188) were enrolled in a longitudinal cohort study and completed a demographic questionnaire, as well as the Brief Pain Inventory, Hospital Depression and Anxiety Scale, Lee Fatigue Scale, Fatigue Severity Scale, and Brief Illness Perception Questionnaire on the day before surgery. Clinical data were extracted from medical records.
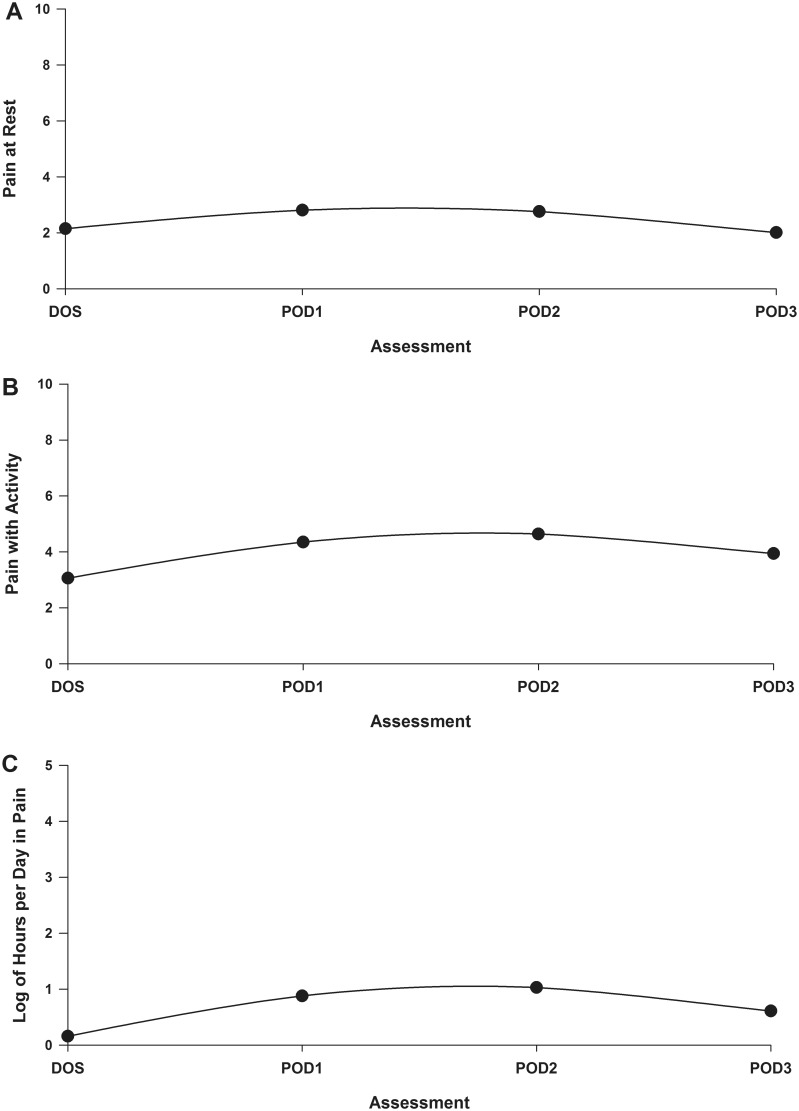
Setting and patients: Each patient completed a pain diary that assessed pain at rest and with activity, and hours per day in pain every evening from day of surgery until postoperative day 3. Using hierarchical linear modeling, we investigated which demographic, clinical, symptom, and psychological characteristics predicted initial levels as well as the trajectories of acute pain at rest and with activity, and hours per day in pain.
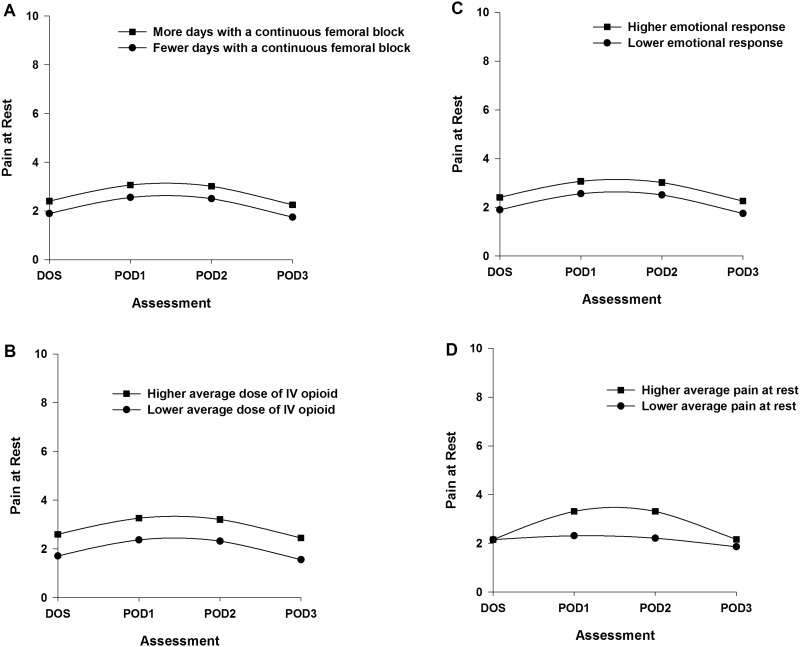
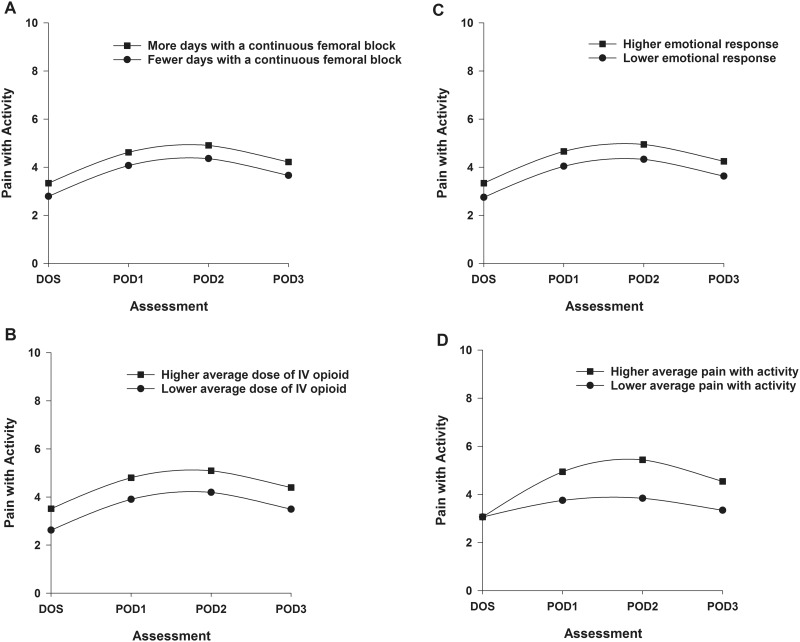
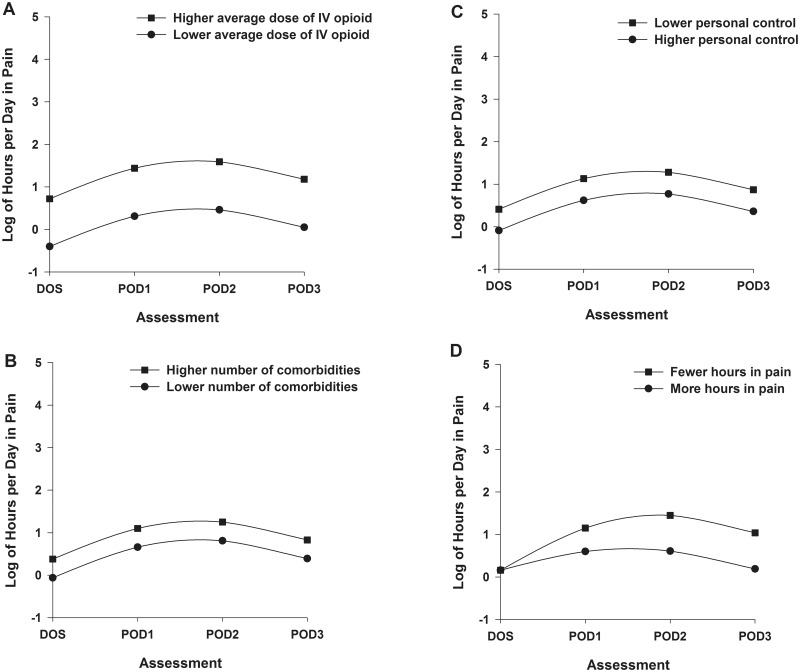
Results: Higher levels of all three acute pain characteristics on the day of surgery resulted in worse trajectories. Higher pain scores with rest and with activity on the day of surgery were associated with more days with femoral block, higher average dose of opioids, and higher emotional response to osteoarthritis. Higher number of comorbidities, higher average dose of opioids, and lower perceived control predicted more hours per day in pain on the day of surgery.
Conclusions: This study identified several potentially modifiable predictors of worsening pain trajectories following total knee arthroplasty. Optimal pain management warrants identification of these high-risk patients and treatment of modifiable risk factors.
Keywords: Acute Postoperative Pain; Hierarchical Linear Modeling; Pain at Rest; Pain with Activity; Total Knee Arthroplasty.
© 2016 American Academy of Pain Medicine.
Figures
Similar articles
-
Preoperative Pain, Symptoms, and Psychological Factors related to Higher Acute Pain Trajectories during Hospitalization for Total Knee Arthroplasty.PLoS One. 2016 Sep 1;11(9):e0161681. doi: 10.1371/journal.pone.0161681. eCollection 2016. PLoS One. 2016. PMID: 27583551 Free PMC article.
-
Factors that can predict pain with walking, 12 months after total knee arthroplasty.Acta Orthop. 2016 Dec;87(6):600-606. doi: 10.1080/17453674.2016.1237440. Epub 2016 Sep 23. Acta Orthop. 2016. PMID: 27658970 Free PMC article.
-
Predictors of acute postsurgical pain and anxiety following primary total hip and knee arthroplasty.J Pain. 2013 May;14(5):502-15. doi: 10.1016/j.jpain.2012.12.020. Epub 2013 Mar 27. J Pain. 2013. PMID: 23541065
-
Management of neuropathic pain after knee surgery.Joint Bone Spine. 2016 Dec;83(6):657-663. doi: 10.1016/j.jbspin.2016.06.001. Epub 2016 Jul 15. Joint Bone Spine. 2016. PMID: 27426445 Review.
-
Predictive Factors for Developing Chronic Pain After Total Knee Arthroplasty.J Arthroplasty. 2018 Nov;33(11):3372-3378. doi: 10.1016/j.arth.2018.07.028. Epub 2018 Aug 4. J Arthroplasty. 2018. PMID: 30143334 Review.
Cited by
-
Factors associated with success and failure of patient-controlled oral analgesia after total hip and knee arthroplasty: a historical comparative cohort study.Can J Anaesth. 2021 Mar;68(3):324-335. doi: 10.1007/s12630-020-01864-5. Epub 2020 Nov 17. Can J Anaesth. 2021. PMID: 33205265 English.
-
Psychometric properties of a short version of Lee Fatigue Scale used as a generic PROM in persons with stroke or osteoarthritis: assessment using a Rasch analysis approach.Health Qual Life Outcomes. 2020 Jun 5;18(1):168. doi: 10.1186/s12955-020-01419-8. Health Qual Life Outcomes. 2020. PMID: 32503548 Free PMC article.
-
Adductor canal block in combination with posterior capsular infiltration on the pain control after TKA.Ir J Med Sci. 2018 May;187(2):465-471. doi: 10.1007/s11845-017-1647-3. Epub 2017 Jul 7. Ir J Med Sci. 2018. PMID: 28687982
-
The Economic Utility of Clinical Psychology in the Multidisciplinary Management of Pain.Front Psychol. 2017 Oct 31;8:1860. doi: 10.3389/fpsyg.2017.01860. eCollection 2017. Front Psychol. 2017. PMID: 29163260 Free PMC article. No abstract available.
-
Acute Pain Is Associated With Chronic Opioid Use After Total Knee Arthroplasty.Reg Anesth Pain Med. 2018 Oct;43(7):705-711. doi: 10.1097/AAP.0000000000000831. Reg Anesth Pain Med. 2018. PMID: 29975257 Free PMC article.
References
-
- Dalury DF, Lieberman JR, Macdonald SJ. Current and innovative pain management techniques in total knee arthroplasty. Instr Course Lect 2011;61:383–8. - PubMed
-
- Andersen LO, Gaarn-Larsen L, Kristensen BB, et al. Subacute pain and function after fast-track hip and knee arthroplasty. Anaesthesia 2009;64(5):508–13. - PubMed
-
- Ranawat AS, Ranawat CS. Pain management and accelerated rehabilitation for total hip and total knee arthroplasty. J Arthroplasty 2007;22(7 Suppl 3):12–5. - PubMed
-
- Wylde V, Rooker J, Halliday L, Blom A. Acute postoperative pain at rest after hip and knee arthroplasty: Severity, sensory qualities and impact on sleep. Orthop Traumatol Surg Res 2011;97(2):139–44. - PubMed
-
- Puolakka PA, Rorarius MG, Roviola M, et al. Persistent pain following knee arthroplasty. Eur J Anaesthesiol 2010;27(5):455–60. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
