

Effect of Oral JZP-110 (ADX-N05) on Wakefulness and Sleepiness in Adults with Narcolepsy: A Phase 2b Study
- PMID: 27166238
- PMCID: PMC4909620
- DOI: 10.5665/sleep.5968
Effect of Oral JZP-110 (ADX-N05) on Wakefulness and Sleepiness in Adults with Narcolepsy: A Phase 2b Study
Abstract
Study objectives: To evaluate the efficacy and safety of oral JZP-110, a second-generation wake-promoting agent with dopaminergic and noradrenergic activity, for treatment of impaired wakefulness and excessive sleepiness in adults with narcolepsy.
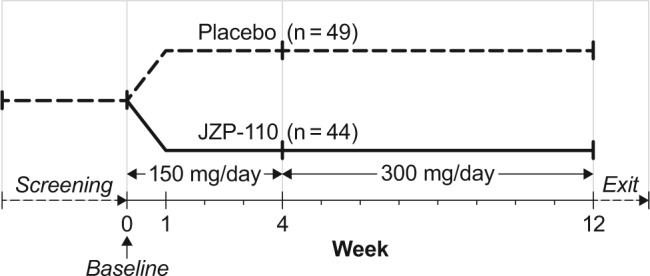
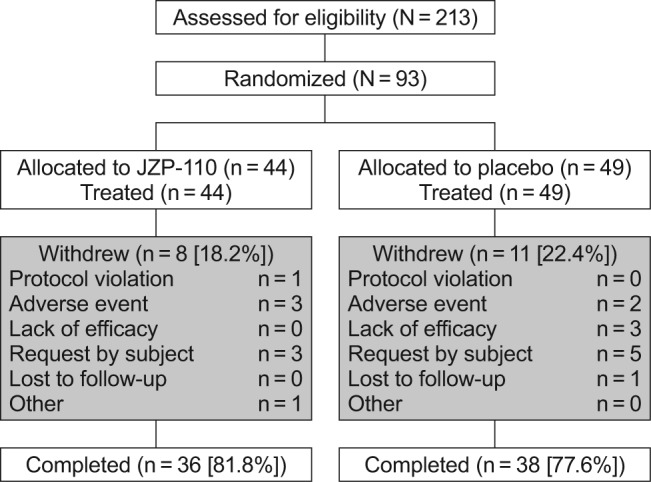
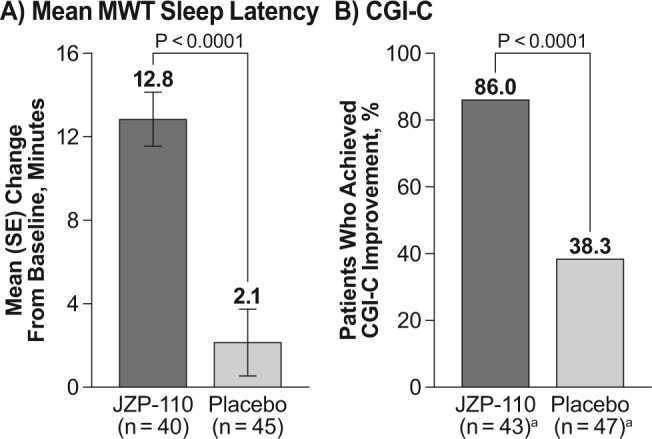
Methods: This was a phase 2b, randomized, double-blind, placebo-controlled, parallel-group trial conducted at 28 centers in the United States. Patients were adults with narcolepsy who had baseline scores ≥ 10 on the Epworth Sleepiness Scale (ESS) and baseline sleep latency ≤ 10 min on the Maintenance of Wakefulness Test (MWT). Patients received a daily placebo (n = 49) or JZP-110 (n = 44) 150 mg/day weeks 1-4 and 300 mg/day weeks 5-12. Primary efficacy endpoints were change from baseline in average MWT sleep latency, and the Clinical Global Impression-Change (CGI-C); secondary endpoints were change from baseline in ESS score and Patient Global Impression-Change.
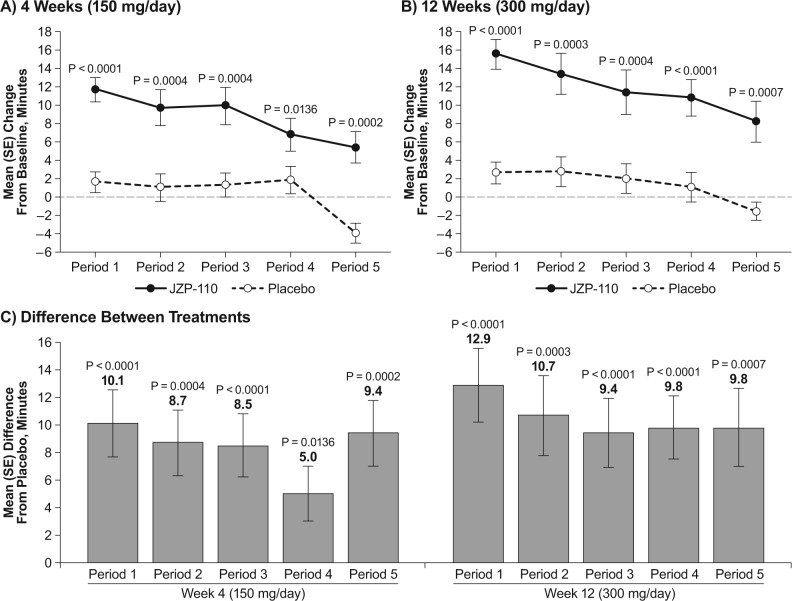
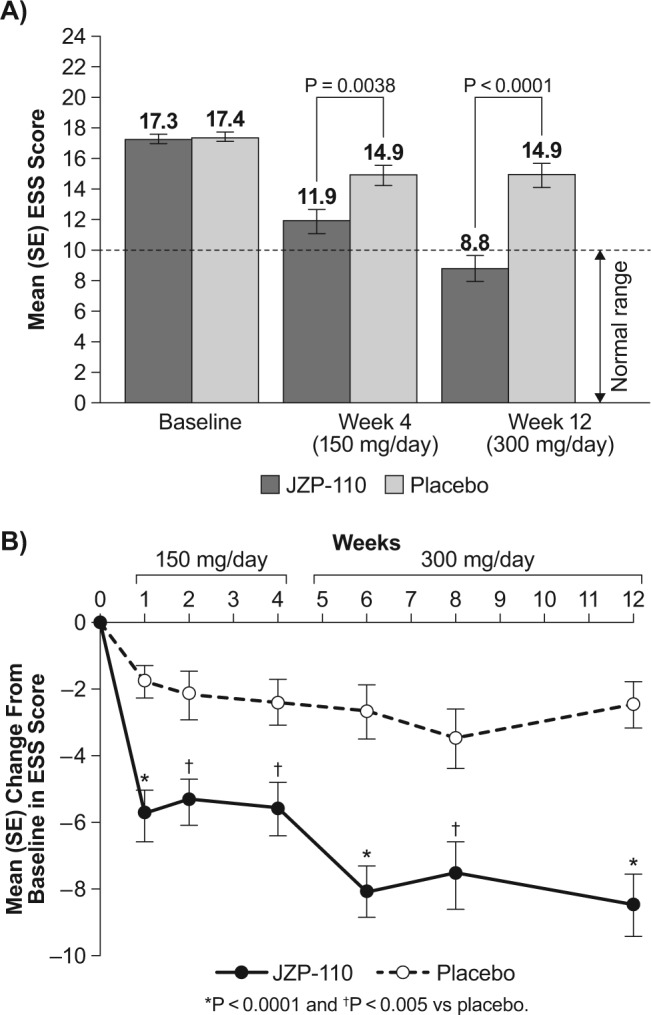
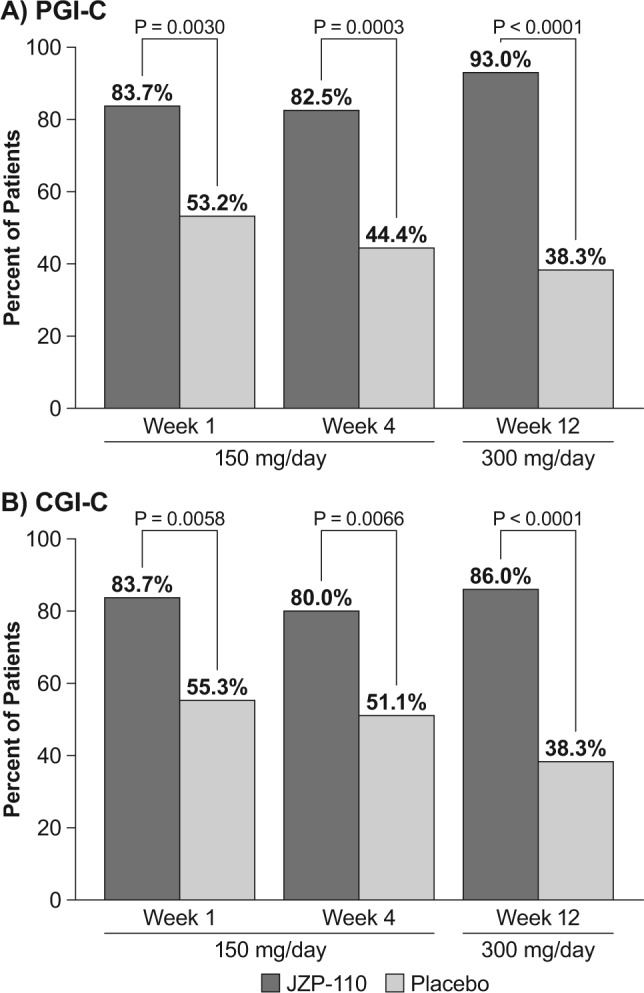
Results: Improvements were significantly greater with JZP-110 versus placebo on mean MWT sleep latency (4 w, 9.5 versus 1.4 min, P < 0.0001; 12 w, 12.8 versus 2.1 min, P < 0.0001), percentage of patients with CGI-C improvement (4 w, 80% versus 51%, P = 0.0066; 12 w, 86% versus 38%, P < 0.0001), and mean change in ESS (4 w, -5.6 versus -2.4, P = 0.0038; 12 w, -8.5 versus -2.5, P < 0.0001). Three JZP-110-treated patients (6.8%) discontinued due to adverse events (AEs). The most common AEs with JZP-110 versus placebo were insomnia (23% versus 8%), headache (16% versus 10%), nausea (14% versus 6%), diarrhea (11% versus 6%), decreased appetite (14% versus 0%), and anxiety (11% versus 0%).
Conclusions: At doses of 150-300 mg/day, JZP-110 was well tolerated and significantly improved the ability to stay awake and subjective symptoms of excessive sleepiness in adults with narcolepsy.
Clinical trials registration: Clinicaltrials.gov identifier NCT01681121.
Keywords: JZP-110; excessive sleepiness; narcolepsy; wakefulness.
© 2016 Associated Professional Sleep Societies, LLC.
Figures
References
-
- American Academy of Sleep Medicine. The International Classification of Sleep Disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
-
- Dodel R, Peter H, Spottke A, et al. Health-related quality of life in patients with narcolepsy. Sleep Med. 2007;8:733–41. - PubMed
-
- Jennum P, Ibsen R, Petersen ER, Knudsen S, Kjellberg J. Health, social, and economic consequences of narcolepsy: a controlled national study evaluating the societal effect on patients and their partners. Sleep Med. 2012;13:1086–93. - PubMed
-
- Black J, Reaven NL, Funk S, et al. The Burden of Narcolepsy Disease (BOND) Study: Healthcare Utilization and Cost Findings. Sleep Med. 2014;15:522–9. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
