

Residual Events during Use of CPAP: Prevalence, Predictors, and Detection Accuracy
- PMID: 27166303
- PMCID: PMC4957193
- DOI: 10.5664/jcsm.6056
Residual Events during Use of CPAP: Prevalence, Predictors, and Detection Accuracy
Abstract
Study objectives: To assess the frequency, severity, and determinants of residual respiratory events during continuous positive airway therapy (CPAP) for obstructive sleep apnea (OSA) as determined by device output.
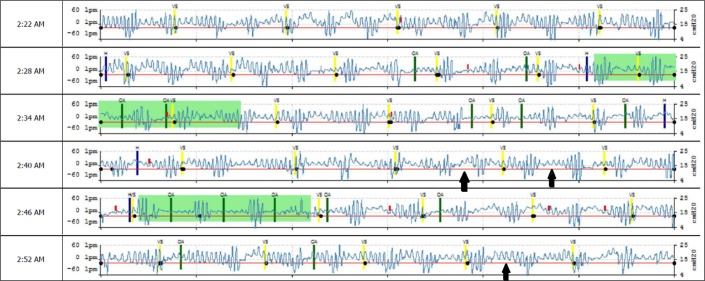
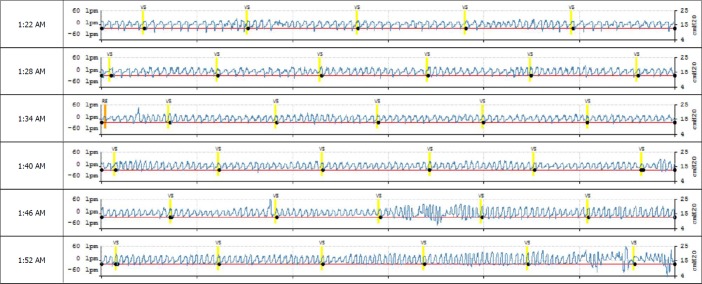
Methods: Subjects were consecutive OSA patients at an American Academy of Sleep Medicine accredited multidisciplinary sleep center. Inclusion criteria included CPAP use for a minimum of 3 months, and a minimum nightly use of 4 hours. Compliance metrics and waveform data from 217 subjects were analyzed retrospectively. Events were scored manually when there was a clear reduction of amplitude (≥ 30%) or flow-limitation with 2-3 larger recovery breaths. Automatically detected versus manually scored events were subjected to statistical analyses included Bland-Altman plots, correlation coefficients, and logistic regression exploring predictors of residual events.
Results: The mean patient age was 54.7 ± 14.2 years; 63% were males. All patients had a primary diagnosis of obstructive sleep apnea, 26% defined as complex sleep apnea. Residual flow measurement based apnea-hypopnea index (AHIFLOW) > 5, 10, and 15/h was seen in 32.3%, 9.7%, and 1.8% vs. 60.8%, 23%, and 7.8% of subjects based on automated vs. manual scoring of waveform data. Automatically detected versus manually scored average AHIFLOW was 4.4 ± 3.8 vs. 7.3 ± 5.1 per hour. In a logistic regression analysis, the only predictors for a manual AHIFLOW > 5/h were the absolute central apnea index (CAI), (odds ratio [OR]: 1.5, p: 0.01, CI: 1.1-2.0), or using a CAI threshold of 5/h of sleep (OR: 5.0, p: < 0.001, CI: 2.2-13.8). For AHIFLOW > 10/h, the OR was 1.14, p: 0.03 (CI: 1.1-1.3) per every CAI unit of 1/hour.
Conclusions: Residual respiratory events are common during CPAP treatment, may be missed by automated device detection and predicted by a high central apnea index on the baseline diagnostic study. Direct visualization of flow data is generally available and improves detection.
Keywords: auto-CPAP; residual apnea; sleep.
© 2016 American Academy of Sleep Medicine.
Figures
References
-
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5. - PubMed
-
- Ikeda Y, Kasai T, Kawana F, et al. Comparison between the apnea-hypopnea indices determined by the REMstar Auto M series and those determined by standard in-laboratory polysomnography in patients with obstructive sleep apnea. Intern Med. 2012;51:2877–85. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
