

Phase 2 study of panobinostat with or without rituximab in relapsed diffuse large B-cell lymphoma
- PMID: 27166360
- PMCID: PMC4972610
- DOI: 10.1182/blood-2016-02-699520
Phase 2 study of panobinostat with or without rituximab in relapsed diffuse large B-cell lymphoma
Abstract
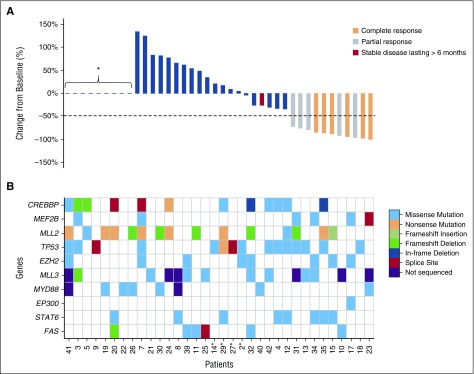
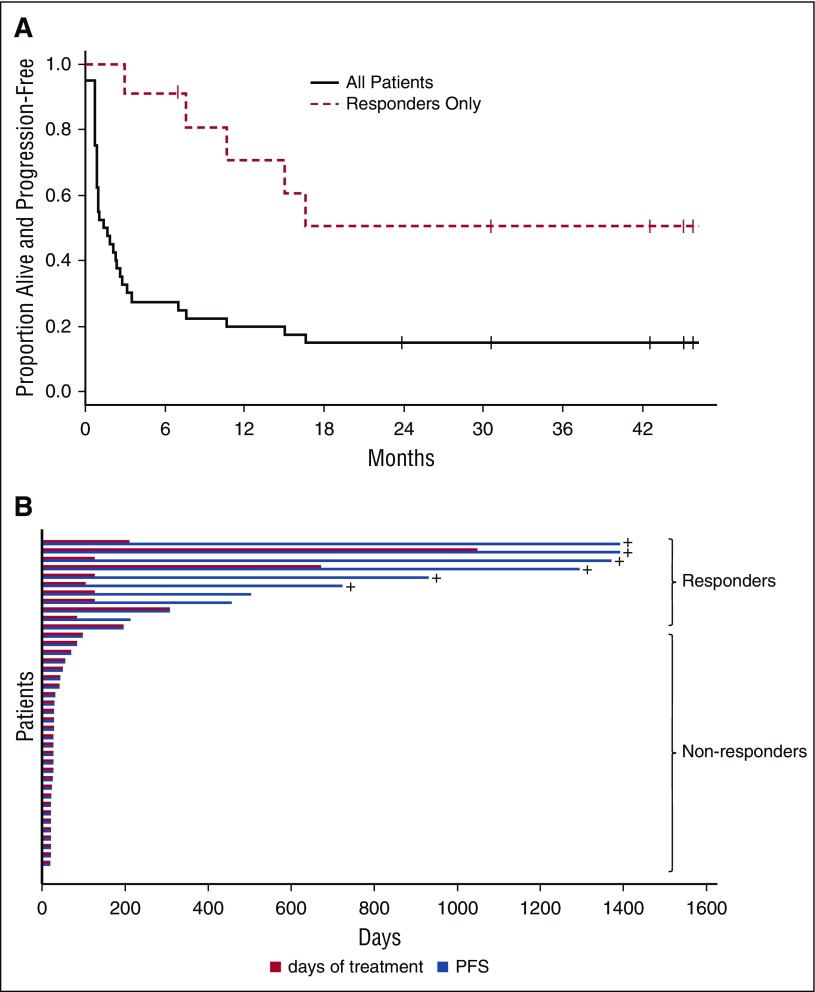
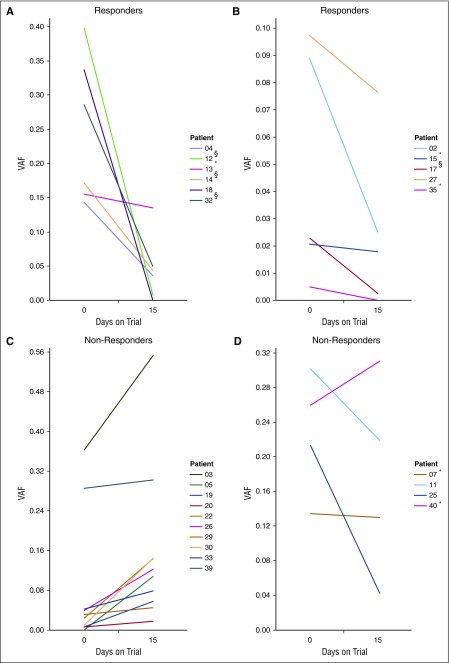
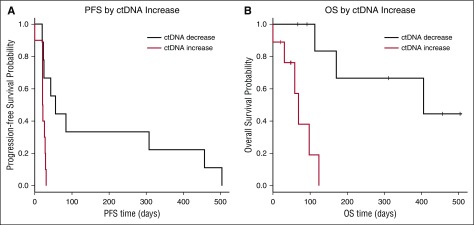
The majority of diffuse large B-cell lymphoma (DLBCL) tumors contain mutations in histone-modifying enzymes (HMEs), indicating a potential therapeutic benefit of histone deacetylase inhibitors (HDIs), and preclinical data suggest that HDIs augment the effect of rituximab. In this randomized phase 2 study, we evaluated the response rate and toxicity of panobinostat, a pan-HDI administered 30 mg orally 3 times weekly, with or without rituximab, in 40 patients with relapsed or refractory de novo (n = 27) or transformed (n = 13) DLBCL. Candidate genes and whole exomes were sequenced in relapse tumor biopsies to search for molecular correlates, and these data were used to quantify circulating tumor DNA (ctDNA) in serial plasma samples. Eleven of 40 patients (28%) responded to panobinostat (95% confidence interval [CI] 14.6-43.9) and rituximab did not increase responses. The median duration of response was 14.5 months (95% CI 9.4 to "not reached"). At time of data censoring, 6 of 11 patients had not progressed. Of the genes tested for mutations, only those in MEF2B were significantly associated with response. We detected ctDNA in at least 1 plasma sample from 96% of tested patients. A significant increase in ctDNA at day 15 relative to baseline was strongly associated with lack of response (sensitivity 71.4%, specificity 100%). We conclude that panobinostat induces very durable responses in some patients with relapsed DLBCL, and early responses can be predicted by mutations in MEF2B or a significant change in ctDNA level at 15 days after treatment initiation. This clinical trial was registered at www.ClinicalTrials.gov (#NCT01238692).
© 2016 by The American Society of Hematology.
Figures
Comment in
-
Precision monitoring takes the stage.Blood. 2016 Jul 14;128(2):149-50. doi: 10.1182/blood-2016-05-717520. Blood. 2016. PMID: 27418622 Free PMC article.
References
-
- Coiffier B, Thieblemont C, Van Den Neste E, et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d’Etudes des Lymphomes de l’Adulte. Blood. 2010;116(12):2040–2045. - PMC - PubMed
-
- Sehn LH, Berry B, Chhanabhai M, et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood. 2007;109(5):1857–1861. - PubMed
-
- Pfreundschuh M, Kuhnt E, Trümper L, et al. MabThera International Trial (MInT) Group. CHOP-like chemotherapy with or without rituximab in young patients with good-prognosis diffuse large-B-cell lymphoma: 6-year results of an open-label randomised study of the MabThera International Trial (MInT) Group. Lancet Oncol. 2011;12(11):1013–1022. - PubMed
-
- Crump M, Kuruvilla J, Couban S, et al. Randomized comparison of gemcitabine, dexamethasone, and cisplatin versus dexamethasone, cytarabine, and cisplatin chemotherapy before autologous stem-cell transplantation for relapsed and refractory aggressive lymphomas: NCIC-CTG LY.12. J Clin Oncol. 2014;32(31):3490–3496. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
