

Nurses versus physician-led interhospital critical care transport: a randomized non-inferiority trial
- PMID: 27166622
- PMCID: PMC4879164
- DOI: 10.1007/s00134-016-4355-y
Nurses versus physician-led interhospital critical care transport: a randomized non-inferiority trial
Abstract
Purpose: Regionalization and concentration of critical care increases the need for interhospital transport. However, optimal staffing of ground critical care transport has not been evaluated.
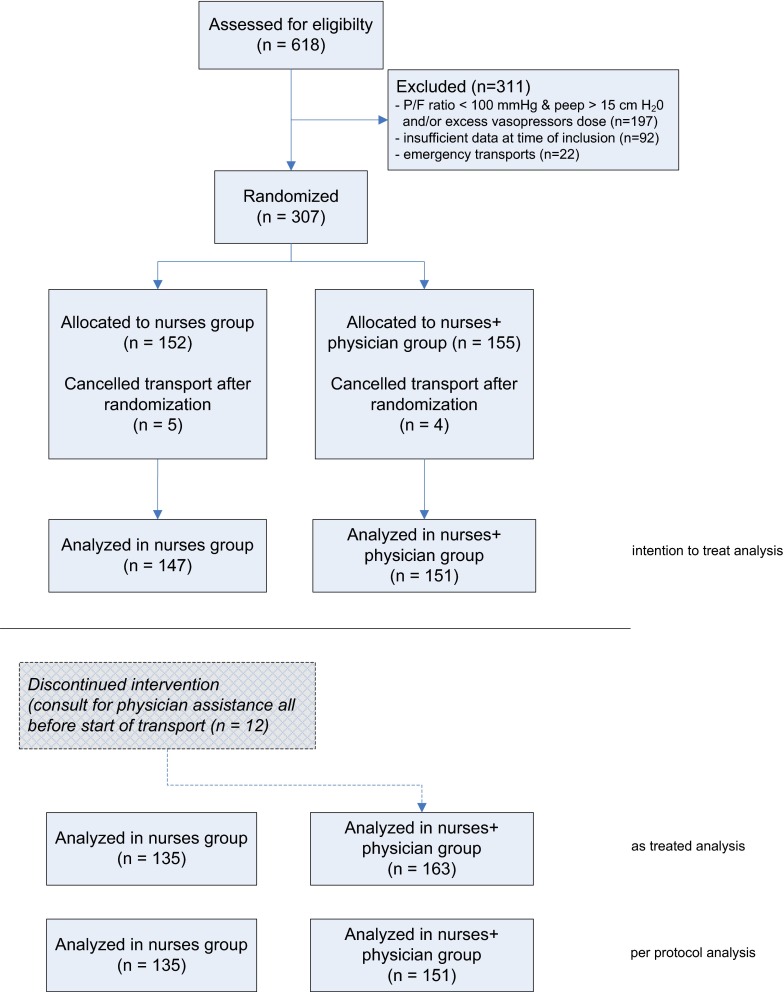
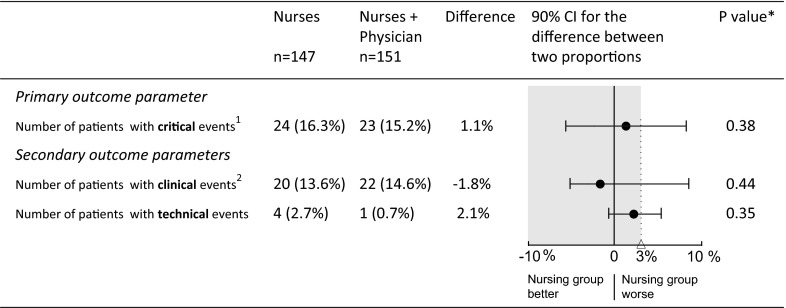
Methods: In this prospective, randomized, open-label, blinded-endpoint non-inferiority trial, critically ill patients on mechanical ventilation transported by interhospital ground critical care transport were randomized between transport staffed by a dedicated team comprising a critical care nurse and paramedic (nurses group) or a dedicated team including a critical care physician (nurses + physician group). The primary outcome was the number of patients with critical events, both clinical and technical, during transport. Clinical events included decrease in blood pressure, oxygen saturation, or temperature, blood loss, new cardiac arrhythmias, or death. Non-inferiority was assumed if the upper limit of the two-sided 90 % confidence interval (CI) for the between-group difference lies below the non-inferiority margin of 3 %.
Results: Of 618 eligible transported critically ill patients, 298 could be analyzed after randomization and allocation to the nurses group (n = 147) or nurses + physician group (n = 151). The percentages of patients with critical events were 16.3 % (24 incidents in 147 transports) in the nurses group and 15.2 % (23 incidents in 151 transports) in the nurses + physician group (difference 1.1 %, two-sided 90 % CI [-5.9 to 8.1]). Critical events occurred in both groups at a higher than the expected (0-1 %) rate. In the nurses group consultations for physician assistance were requested in 8.2 % (12 in 147 transports), all of which were performed prior to transport.
Conclusions: The number of patients with critical events did not markedly differ between critical care transports staffed by a critical care nurse and paramedic compared to a team including a critical care physician. However, as a result of an unexpected higher rate of critical events in both groups recorded by an electronic health record, non-inferiority of nurse-led interhospital critical transport could not be established ( http://www.controlled-trials.com/ISRCTN39701540 ).
Keywords: Critical care transport; Interhospital; Mobile intensive care unit; Patient transfer.
Figures
Similar articles
-
Interhospital transport of the extremely ill patient: the mobile intensive care unit.Crit Care Med. 2000 Jan;28(1):79-85. doi: 10.1097/00003246-200001000-00013. Crit Care Med. 2000. PMID: 10667503
-
Critical care interhospital transports: predictability of the need for a pediatrician.Pediatr Emerg Care. 1990 Jun;6(2):89-92. doi: 10.1097/00006565-199006000-00004. Pediatr Emerg Care. 1990. PMID: 2371162
-
Quality of interhospital transport of the critically ill: impact of a Mobile Intensive Care Unit with a specialized retrieval team.Crit Care. 2011;15(1):R75. doi: 10.1186/cc10064. Epub 2011 Feb 28. Crit Care. 2011. PMID: 21356054 Free PMC article.
-
The Importance of Ground Critical Care Transport.J Intensive Care Med. 2017 Feb;32(2):163-169. doi: 10.1177/0885066616668484. Epub 2016 Sep 22. J Intensive Care Med. 2017. PMID: 27625421 Review.
-
Transport of critically ill patients.J Intensive Care Med. 1992 Sep-Oct;7(5):223-33. doi: 10.1177/088506669200700503. J Intensive Care Med. 1992. PMID: 10147941 Review.
Cited by
-
Comparison of patient characteristics and long-term mortality between transferred and non-transferred COVID-19 patients in Dutch intensive care units: A national cohort study.Acta Anaesthesiol Scand. 2022 Oct;66(9):1107-1115. doi: 10.1111/aas.14129. Epub 2022 Aug 28. Acta Anaesthesiol Scand. 2022. PMID: 36031794 Free PMC article.
-
Collective Critical Care Ambulance: an innovative transportation of critical care patients by bus in COVID-19 pandemic response.Scand J Trauma Resusc Emerg Med. 2021 Jun 4;29(1):78. doi: 10.1186/s13049-021-00896-0. Scand J Trauma Resusc Emerg Med. 2021. PMID: 34088335 Free PMC article.
-
Emergency critical care: closing the gap between onset of critical illness and intensive care unit admission.Wien Klin Wochenschr. 2024 Dec;136(23-24):651-661. doi: 10.1007/s00508-024-02374-w. Epub 2024 May 16. Wien Klin Wochenschr. 2024. PMID: 38755419 Free PMC article. Review.
-
Interhospital critical care transports: a safe trip indeed!Intensive Care Med. 2016 Nov;42(11):1837. doi: 10.1007/s00134-016-4521-2. Epub 2016 Sep 12. Intensive Care Med. 2016. PMID: 27620290 No abstract available.
-
The association of intensive care capacity transfers with survival in COVID-19 patients from a Scottish district general hospital: A retrospective cohort study.J Intensive Care Soc. 2023 Aug;24(3):277-282. doi: 10.1177/17511437221111638. Epub 2022 Oct 8. J Intensive Care Soc. 2023. PMID: 37744069 Free PMC article.
References
-
- Ramnarayan P, Thiru K, Parslow RC, Harrison DA, Draper ES, Rowan KM. Effect of specialist retrieval teams on outcomes in children admitted to paediatric intensive care units in England and Wales: a retrospective cohort study. Lancet. 2010;376:698–704. doi: 10.1016/S0140-6736(10)61113-0. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
