

Neurotization of free gracilis transfer with the brachialis branch of the musculocutaneous nerve to restore finger and thumb flexion in lower trunk brachial plexus injury: an anatomical study and case report
- PMID: 27166768
- PMCID: PMC4825193
- DOI: 10.6061/clinics/2016(04)03
Neurotization of free gracilis transfer with the brachialis branch of the musculocutaneous nerve to restore finger and thumb flexion in lower trunk brachial plexus injury: an anatomical study and case report
Abstract
Objective: To investigate the feasibility of using free gracilis muscle transfer along with the brachialis muscle branch of the musculocutaneous nerve to restore finger and thumb flexion in lower trunk brachial plexus injury according to an anatomical study and a case report.
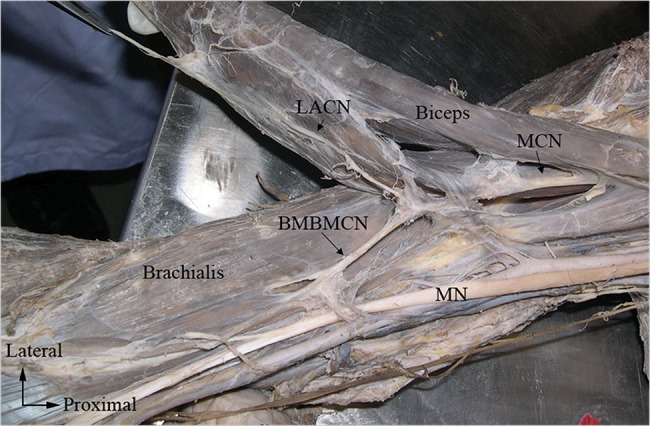
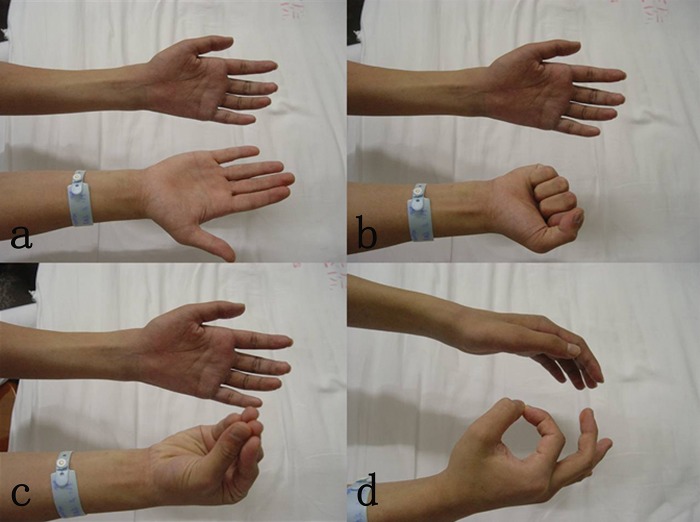
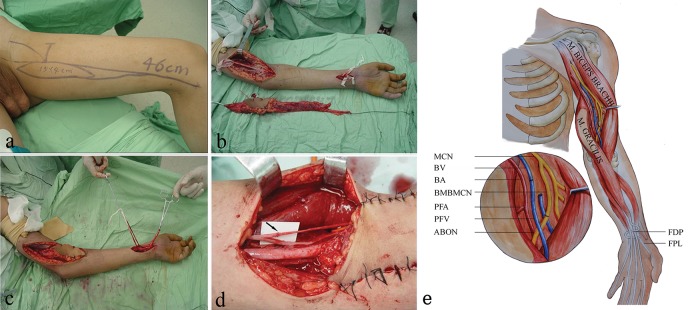
Methods: Thirty formalin-fixed upper extremities from 15 adult cadavers were used in this study. The distance from the point at which the brachialis muscle branch of the musculocutaneous nerve originates to the midpoint of the humeral condylar was measured, as well as the length, diameter, course and branch type of the brachialis muscle branch of the musculocutaneous nerve. An 18-year-old male who sustained an injury to the left brachial plexus underwent free gracilis transfer using the brachialis muscle branch of the musculocutaneous nerve as the donor nerve to restore finger and thumb flexion. Elbow flexion power and hand grip strength were recorded according to British Medical Research Council standards. Postoperative measures of the total active motion of the fingers were obtained monthly.
Results: The mean length and diameter of the brachialis muscle branch of the musculocutaneous nerve were 52.66±6.45 and 1.39±0.09 mm, respectively, and three branching types were observed. For the patient, the first gracilis contraction occurred during the 4th month. A noticeable improvement was observed in digit flexion one year later; the muscle power was M4, and the total active motion of the fingers was 209°.
Conclusions: Repairing injury to the lower trunk of the brachial plexus by transferring the brachialis muscle branch of the musculocutaneous nerve to the anterior branch of the obturator nerve using a tension-free direct suture is technically feasible, and the clinical outcome was satisfactory in a single surgical patient.
Conflict of interest statement
No potential conflict of interest was reported.
Figures



Similar articles
-
Repair of brachial plexus lower trunk injury by transferring brachialis muscle branch of musculocutaneous nerve: anatomic feasibility and clinical trials.Chin Med J (Engl). 2008 Jan 20;121(2):99-104. Chin Med J (Engl). 2008. PMID: 18272032
-
Free Functioning Gracilis Muscle Transfer With and Without Simultaneous Intercostal Nerve Transfer to Musculocutaneous Nerve for Restoration of Elbow Flexion After Traumatic Adult Brachial Pan-Plexus Injury.J Hand Surg Am. 2017 Apr;42(4):293.e1-293.e7. doi: 10.1016/j.jhsa.2017.01.014. Epub 2017 Feb 27. J Hand Surg Am. 2017. PMID: 28249790
-
Transfer of brachialis branch of musculocutaneous nerve for finger flexion: anatomic study and case report.Microsurgery. 2004;24(5):358-62. doi: 10.1002/micr.20053. Microsurgery. 2004. PMID: 15378580
-
Single-stage double motor nerve transfer for all finger flexion in iatrogenic C8-T1 spinal nerve injury: a case report and review of literature.Acta Neurochir (Wien). 2022 Oct;164(10):2683-2688. doi: 10.1007/s00701-022-05264-0. Epub 2022 Jun 4. Acta Neurochir (Wien). 2022. PMID: 35660975 Review.
-
Factors Affecting Outcomes After Free Functional Gracilis Muscle Transfer for Elbow Flexion in Brachial Plexus Injury: A Systematic Review and Meta-Analysis.J Hand Surg Am. 2024 Dec;49(12):1173-1185. doi: 10.1016/j.jhsa.2024.07.012. Epub 2024 Sep 2. J Hand Surg Am. 2024. PMID: 39230552
Cited by
-
[Construction of Chinese peripheral nerve society and progress in repair and reconstruction of peripheral nerve injury].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018 Jul 15;32(7):786-791. doi: 10.7507/1002-1892.201807020. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018. PMID: 30129296 Free PMC article. Chinese.
-
Hand reanimation: functional free gracilis transfer or transfer of the distal tendon of the biceps to the flexor digitorum profundus and flexor pollicis longus as surgical options.Einstein (Sao Paulo). 2024 Nov 8;22:eAO0719. doi: 10.31744/einstein_journal/2024AO0719. eCollection 2024. Einstein (Sao Paulo). 2024. PMID: 39536210 Free PMC article.
-
Transfer of the anterior branch of the obturator nerve for femoral nerve reconstruction and preservation of motor function: A case report.Int J Surg Case Rep. 2018;51:58-61. doi: 10.1016/j.ijscr.2018.08.004. Epub 2018 Aug 9. Int J Surg Case Rep. 2018. PMID: 30144711 Free PMC article.
-
Repair of peripheral nerve defects by nerve transposition using small gap bio-sleeve suture with different inner diameters at both ends.Neural Regen Res. 2019 Apr;14(4):706-712. doi: 10.4103/1673-5374.247475. Neural Regen Res. 2019. PMID: 30632512 Free PMC article.
References
-
- Terzis JK, Kostas I, Soucacos PN. Restoration of shoulder function with nerve transfers in traumatic brachial plexus palsy patients. Microsurgery. 2006;26((4)):316–24. 10.1002/micr.20245 - DOI - PubMed
-
- Tu YK, Tsai YJ, Chang CH, Su FC, Hsiao CK, Tan JS. Surgical treatment for total root avulsion type brachial plexus injuries by neurotization: a prospective comparison study between total and hemicontralateral C7 nerve root transfer. Microsurgery. 2014;34((2)):91–101. 10.1002/micr.22148 - DOI - PMC - PubMed
-
- Tsai YJ, Su FC, Hsiao CK, Tu YK. Comparison of objective muscle strength in C5-C6 and C5-C7 brachial plexus injury patients after double nerve transfer. Microsurgery. 2015;35((2)):107–14. 10.1002/micr.22283 - DOI - PubMed
-
- Bertelli JA, Ghizoni MF. Transfer of supinator motor branches to the posterior interosseous nerve in C7-T1 brachial plexus palsy. J Neurosurg. 2010;113((1)):129–32. 10.3171/2009.10.JNS09854 - DOI - PubMed
-
- Yang J, Jia X, Yu C, Gu Y. Pronator teres branch transfer to the anterior interosseous nerve for treating C8T1 brachial plexus avulsion: an anatomic study and case report. Neurosurgery. 2014;75((4)):375–9. 10.1227/NEU.0000000000000435 discussion 379. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
