

Comparison of manual and automatic MR-CT registration for radiotherapy of prostate cancer
- PMID: 27167285
- PMCID: PMC5690943
- DOI: 10.1120/jacmp.v17i3.6088
Comparison of manual and automatic MR-CT registration for radiotherapy of prostate cancer
Abstract
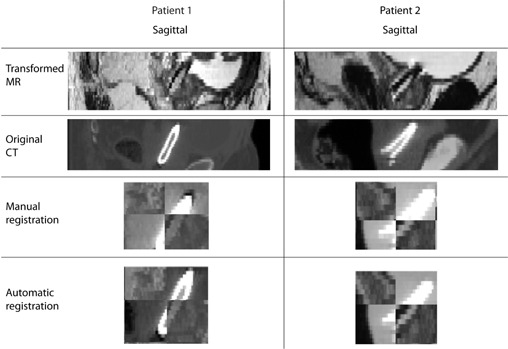
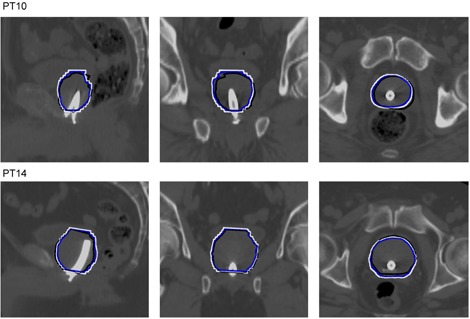
In image-guided radiotherapy (IGRT) of prostate cancer, delineation of the clini-cal target volume (CTV) often relies on magnetic resonance (MR) because of its good soft-tissue visualization. Registration of MR and computed tomography (CT) is required in order to add this accurate delineation to the dose planning CT. An automatic approach for local MR-CT registration of the prostate has previously been developed using a voxel property-based registration as an alternative to a manual landmark-based registration. The aim of this study is to compare the two registration approaches and to investigate the clinical potential for replacing the manual registration with the automatic registration. Registrations and analysis were performed for 30 prostate cancer patients treated with IGRT using a Ni-Ti prostate stent as a fiducial marker. The comparison included computing translational and rotational differences between the approaches, visual inspection, and computing the overlap of the CTV. The computed mean translational difference was 1.65, 1.60, and 1.80mm and the computed mean rotational difference was 1.51°, 3.93°, and 2.09° in the superior/inferior, anterior/posterior, and medial/lateral direction, respectively. The sensitivity of overlap was 87%. The results demonstrate that the automatic registration approach performs registrations comparable to the manual registration.
Figures

References
-
- Gao Z, Wilkins D, Eapen L, Morash C, Wassef Y, Gerig L. A study of prostate delineation referenced against a gold standard created from the visible human data. Radiother Oncol. 2007;85(2):239–46. - PubMed
-
- Hentschel B, Oehler W, Strauβ D, Ulrich A, Malich A. Definition of the CTV prostate in CT and MRI by using CT‐MRI image fusion in IMRT planning for prostate cancer. Strahlenther Onkol. 2011;187(3):183–90. - PubMed
-
- Rasch C, Barillot I, Remeijer P, van Herk M, Lebesque JV. Definition of the prostate in CT and MRI: a multiobserver study. Int J Radiat Oncol Biol Phys. 1999;43(1):57–66. - PubMed
-
- Langen KM and Jones DTL. Organ motion and its management. Int J Radiat Oncol Biol Phys. 2001;50(1):265–78. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
