

Implications of Multiple Complications on the Postoperative Recovery of General Surgery Patients
- PMID: 27167563
- PMCID: PMC6214627
- DOI: 10.1097/SLA.0000000000001390
Implications of Multiple Complications on the Postoperative Recovery of General Surgery Patients
Abstract
Objectives: To evaluate the association between multiple complications and postoperative outcomes and to assess which complications occur together in patients with multiple complications.
Background: Patients who suffer multiple complications have increased risk of prolonged hospital stay and mortality. However, little is known about what places patients at risk for multiple complications or which complications tend to occur in these patients.
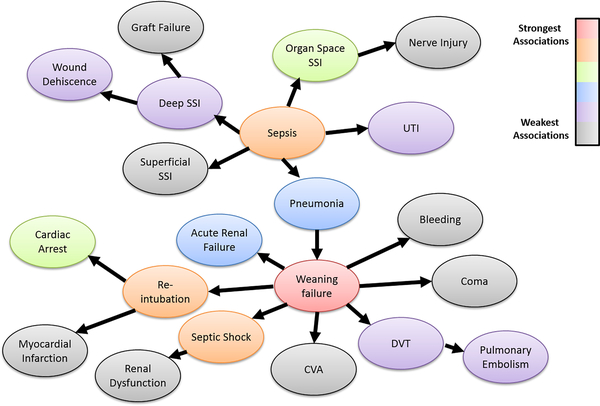
Methods: Surgical patients were identified from the American College of Surgeons National Quality Improvement Program (ACS NSQIP) database from 2005 to 2011. The frequency of postoperative complications was assessed. Patients with less than two complications were compared with patients who had multiple complications using χ and logistic regression analysis. Relationships among postoperative complications were explored by learning a Bayesian network model.
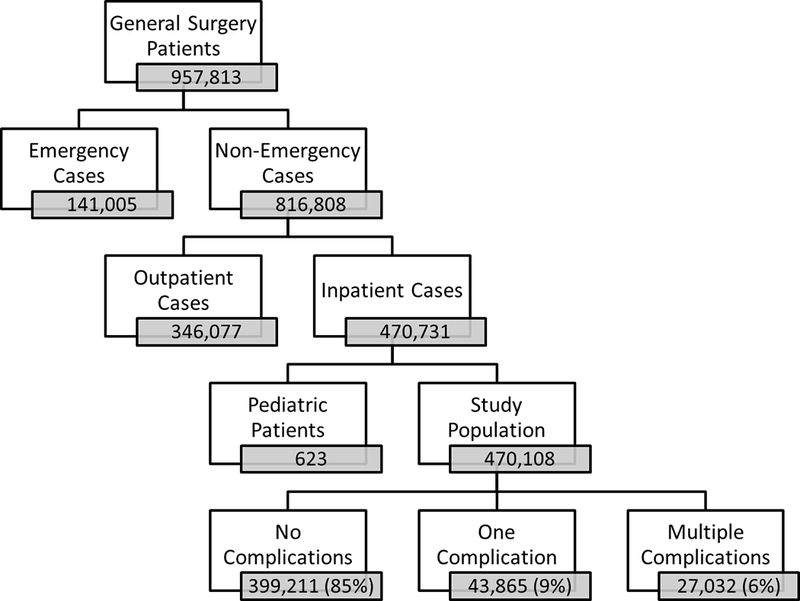
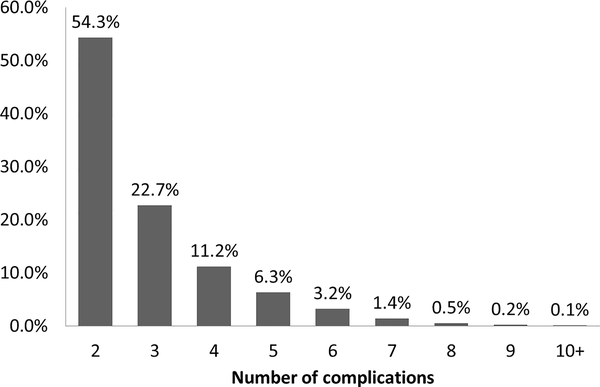
Results: The study population consisted of 470,108 general surgery patients. The overall complication rate was 15% with multiple complications in 27,032 (6%) patients. Patients with multiple complications had worse postoperative outcomes (P < 0.001). The strongest predictors for developing multiple complications were admission from chronic care facility or nursing home, dependent functional status, and higher American Society of Anesthesiologist Physical Status classification. In patients with multiple complications, the most common complication was sepsis (42%), followed by failure to wean ventilator (31%), and organ space surgical site infection (27%). We found that severe complications were most strongly associated with development of multiple complications. Using a Bayesian network, we were able to identify how strongly associated specific complications were in patients who developed multiple complications.
Conclusions: Almost half (40%) of patients with complications suffer multiple complications. Patient factors such as frailty and comorbidity strongly predict the development of multiple complications. The results of our Bayesian analysis identify targets for interventions aimed at disrupting the cascade of multiple complications in high-risk patients.
Conflict of interest statement
The authors have no conflicts of interest to report.
Figures

References
-
- Longo WE, Virgo KS, Johnson FE, et al. Risk factors for Morbidity and Mortality After Colectomy for Colon Cancer. Diseases of the Colon and Rectum. 2000;43:83–91. - PubMed
-
- Mayo NE, Feldman L, Scott S, et al. Impact of preoperative change in physical function on postoperative recovery: Argument supporting prehabilitation for colorectal surgery. Surgery. 2011;2011:505–514. - PubMed
-
- Strasberg SM, Hall BL. Postoperative morbidity index: a quantitative measure of severity of postoperative complications. J Am Coll Surg. 2011;213:616–626. - PubMed
-
- Cohen ME, Bilimoria KY, Ko CY, Hall BL. Development of an American College of Surgeons National Surgery Quality Improvement Program: morbidity and mortality risk calculator for colorectal surgery. J Am Coll Surg. 2009;208:1009–1016. - PubMed
-
- Ghaferi AA, Osborne NH, Birkmeyer JD, Dimick JB. Hospital characteristics associated with failure to rescue from complications after pancreatectomy. J Am Coll Surg. 2010;211:325–330. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
