

Clinical Significance of Symptoms in Smokers with Preserved Pulmonary Function
- PMID: 27168432
- PMCID: PMC4968204
- DOI: 10.1056/NEJMoa1505971
Clinical Significance of Symptoms in Smokers with Preserved Pulmonary Function
Abstract
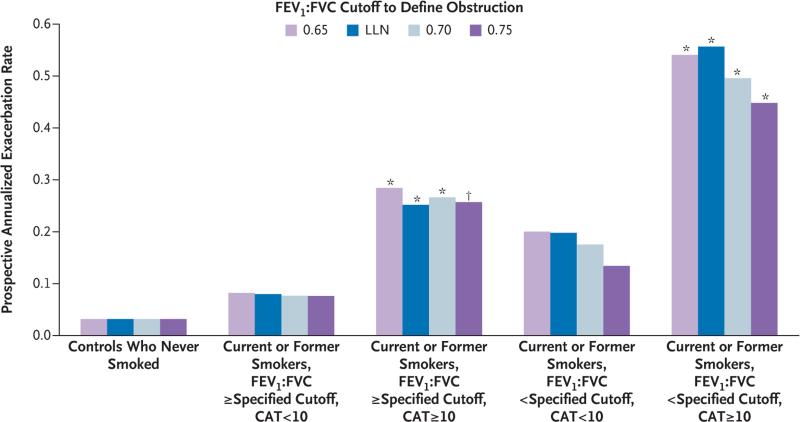
Background: Currently, the diagnosis of chronic obstructive pulmonary disease (COPD) requires a ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) of less than 0.70 as assessed by spirometry after bronchodilator use. However, many smokers who do not meet this definition have respiratory symptoms.
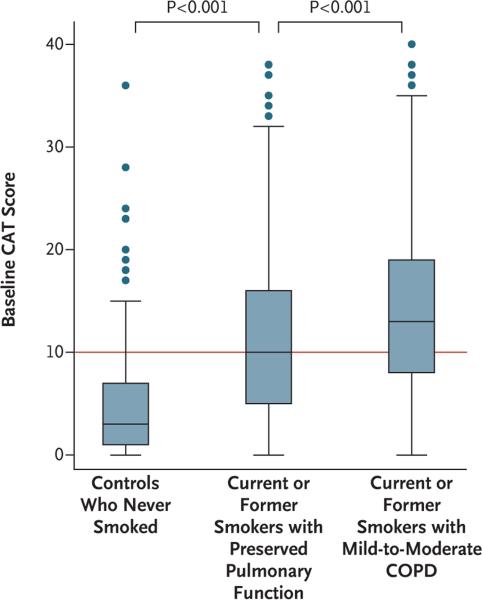
Methods: We conducted an observational study involving 2736 current or former smokers and controls who had never smoked and measured their respiratory symptoms using the COPD Assessment Test (CAT; scores range from 0 to 40, with higher scores indicating greater severity of symptoms). We examined whether current or former smokers who had preserved pulmonary function as assessed by spirometry (FEV1:FVC ≥0.70 and an FVC above the lower limit of the normal range after bronchodilator use) and had symptoms (CAT score, ≥10) had a higher risk of respiratory exacerbations than current or former smokers with preserved pulmonary function who were asymptomatic (CAT score, <10) and whether those with symptoms had different findings from the asymptomatic group with respect to the 6-minute walk distance, lung function, or high-resolution computed tomographic (HRCT) scan of the chest.
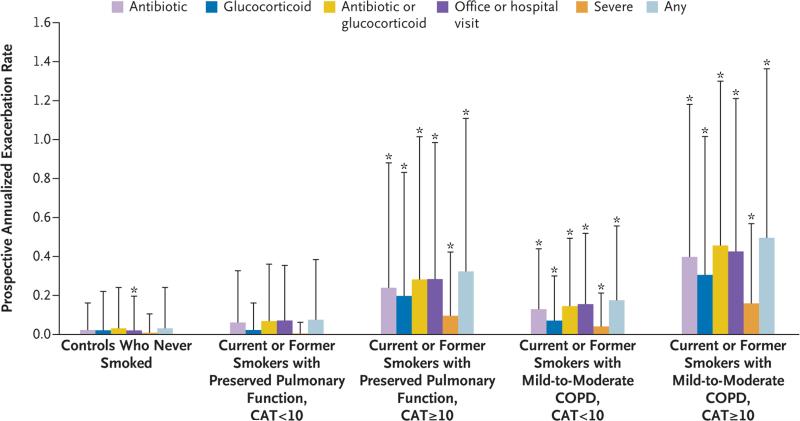
Results: Respiratory symptoms were present in 50% of current or former smokers with preserved pulmonary function. The mean (±SD) rate of respiratory exacerbations among symptomatic current or former smokers was significantly higher than the rates among asymptomatic current or former smokers and among controls who never smoked (0.27±0.67 vs. 0.08±0.31 and 0.03±0.21 events, respectively, per year; P<0.001 for both comparisons). Symptomatic current or former smokers, regardless of history of asthma, also had greater limitation of activity, slightly lower FEV1, FVC, and inspiratory capacity, and greater airway-wall thickening without emphysema according to HRCT than did asymptomatic current or former smokers. Among symptomatic current or former smokers, 42% used bronchodilators and 23% used inhaled glucocorticoids.
Conclusions: Although they do not meet the current criteria for COPD, symptomatic current or former smokers with preserved pulmonary function have exacerbations, activity limitation, and evidence of airway disease. They currently use a range of respiratory medications without any evidence base. (Funded by the National Heart, Lung, and Blood Institute and the Foundation for the National Institutes of Health; SPIROMICS ClinicalTrials.gov number, NCT01969344.).
Figures
Comment in
-
Smoking, Not COPD, as the Disease.N Engl J Med. 2016 May 12;374(19):1885-6. doi: 10.1056/NEJMe1515508. N Engl J Med. 2016. PMID: 27168438 No abstract available.
-
Smokers with respiratory symptoms but no airflow limitation, often have activity limitation, exacerbations and evidence of airway disease.Evid Based Med. 2016 Oct;21(5):189. doi: 10.1136/ebmed-2016-110501. Epub 2016 Aug 23. Evid Based Med. 2016. PMID: 27555639 No abstract available.
-
Symptoms in Smokers with Preserved Pulmonary Function.N Engl J Med. 2016 Sep 1;375(9):897. doi: 10.1056/NEJMc1608235. N Engl J Med. 2016. PMID: 27579643 No abstract available.
-
Symptoms in Smokers with Preserved Pulmonary Function.N Engl J Med. 2016 Sep 1;375(9):895. doi: 10.1056/NEJMc1608235. N Engl J Med. 2016. PMID: 27579644 No abstract available.
-
Symptoms in Smokers with Preserved Pulmonary Function.N Engl J Med. 2016 Sep 1;375(9):895-6. doi: 10.1056/NEJMc1608235. N Engl J Med. 2016. PMID: 27579645 No abstract available.
-
Symptoms in Smokers with Preserved Pulmonary Function.N Engl J Med. 2016 Sep 1;375(9):896. doi: 10.1056/NEJMc1608235. N Engl J Med. 2016. PMID: 27579646 No abstract available.
-
Symptoms in Smokers with Preserved Pulmonary Function.N Engl J Med. 2016 Sep 1;375(9):896-7. doi: 10.1056/NEJMc1608235. N Engl J Med. 2016. PMID: 27606380 No abstract available.
-
Evaluation of symptomatic patients without airflow obstruction: back to the future.J Thorac Dis. 2016 Dec;8(12):E1657-E1660. doi: 10.21037/jtd.2016.12.103. J Thorac Dis. 2016. PMID: 28149607 Free PMC article. No abstract available.
-
Smokers with Normal Spirometry: Impact of Computed Tomography-detected Emphysema, Functional Mechanisms of Dyspnea, and Clinical Significance of Symptoms.Am J Respir Crit Care Med. 2018 Oct 15;198(8):1085-1087. doi: 10.1164/rccm.201711-2256RR. Am J Respir Crit Care Med. 2018. PMID: 30134118 No abstract available.
References
-
- Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347–65. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- HHSN268200900019C/HL/NHLBI NIH HHS/United States
- HHSN268200900009C/WH/WHI NIH HHS/United States
- S10 OD018526/OD/NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- K12 HL119997/HL/NHLBI NIH HHS/United States
- HHSN268200900015C/HL/NHLBI NIH HHS/United States
- I01 CX000911/CX/CSRD VA/United States
- HHSN268200900018C/HL/NHLBI NIH HHS/United States
- HHSN268200900014C/HL/NHLBI NIH HHS/United States
- R01 HL095372/HL/NHLBI NIH HHS/United States
- HHSN268200900016C/HL/NHLBI NIH HHS/United States
- R01 HL110906/HL/NHLBI NIH HHS/United States
- HHSN268200900017C/HL/NHLBI NIH HHS/United States
- HHSN268200900020C/HL/NHLBI NIH HHS/United States
- HHSN268200900013C/HL/NHLBI NIH HHS/United States
- HHSN2682009000019C/PHS HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous