

Patterns of Growth and Decline in Lung Function in Persistent Childhood Asthma
- PMID: 27168434
- PMCID: PMC5032024
- DOI: 10.1056/NEJMoa1513737
Patterns of Growth and Decline in Lung Function in Persistent Childhood Asthma
Abstract
Background: Tracking longitudinal measurements of growth and decline in lung function in patients with persistent childhood asthma may reveal links between asthma and subsequent chronic airflow obstruction.
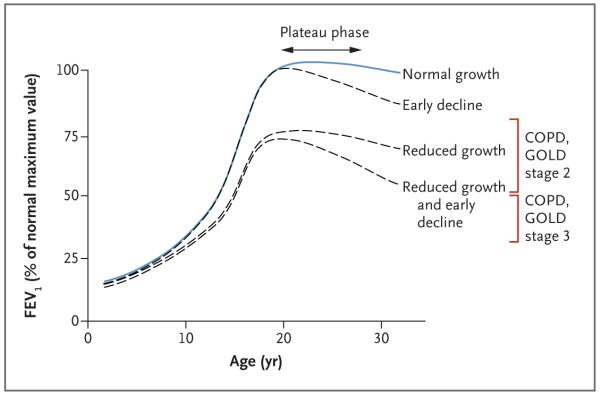
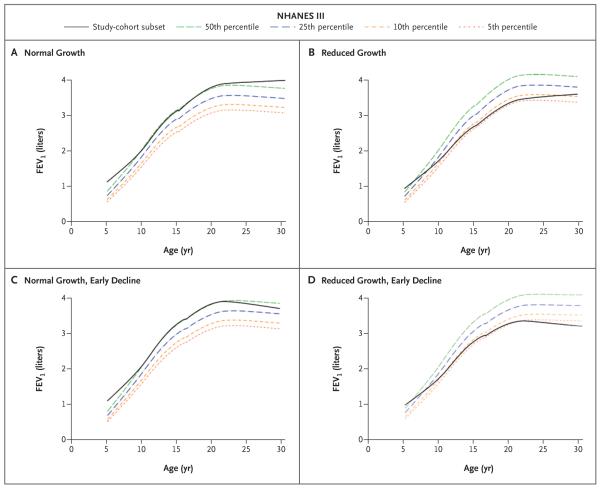
Methods: We classified children with asthma according to four characteristic patterns of lung-function growth and decline on the basis of graphs showing forced expiratory volume in 1 second (FEV1), representing spirometric measurements performed from childhood into adulthood. Risk factors associated with abnormal patterns were also examined. To define normal values, we used FEV1 values from participants in the National Health and Nutrition Examination Survey who did not have asthma.
Results: Of the 684 study participants, 170 (25%) had a normal pattern of lung-function growth without early decline, and 514 (75%) had abnormal patterns: 176 (26%) had reduced growth and an early decline, 160 (23%) had reduced growth only, and 178 (26%) had normal growth and an early decline. Lower baseline values for FEV1, smaller bronchodilator response, airway hyperresponsiveness at baseline, and male sex were associated with reduced growth (P<0.001 for all comparisons). At the last spirometric measurement (mean [±SD] age, 26.0±1.8 years), 73 participants (11%) met Global Initiative for Chronic Obstructive Lung Disease spirometric criteria for lung-function impairment that was consistent with chronic obstructive pulmonary disease (COPD); these participants were more likely to have a reduced pattern of growth than a normal pattern (18% vs. 3%, P<0.001).
Conclusions: Childhood impairment of lung function and male sex were the most significant predictors of abnormal longitudinal patterns of lung-function growth and decline. Children with persistent asthma and reduced growth of lung function are at increased risk for fixed airflow obstruction and possibly COPD in early adulthood. (Funded by the Parker B. Francis Foundation and others; ClinicalTrials.gov number, NCT00000575.).
Figures
Comment in
-
Decline in Lung Function in Childhood Asthma.N Engl J Med. 2016 Aug 18;375(7):e13. doi: 10.1056/NEJMc1608228. N Engl J Med. 2016. PMID: 27532852 No abstract available.
-
Decline in Lung Function in Childhood Asthma.N Engl J Med. 2016 Aug 18;375(7):e13. doi: 10.1056/NEJMc1608228. N Engl J Med. 2016. PMID: 27532853 No abstract available.
-
Decline in Lung Function in Childhood Asthma.N Engl J Med. 2016 Aug 18;375(7):e13. doi: 10.1056/NEJMc1608228. N Engl J Med. 2016. PMID: 27532854 No abstract available.
-
Asthma „verwächst“ sich leider nicht.MMW Fortschr Med. 2017 Jul;159(13):36. doi: 10.1007/s15006-017-9896-7. MMW Fortschr Med. 2017. PMID: 28718122 German. No abstract available.
References
-
- Speizer FE, Tager IB. Epidemiology of chronic mucus hypersecretion and obstructive airways disease. Epidemiol Rev. 1979;1:124–42. - PubMed
-
- Weiss ST, Speizer FE. Epidemiology and natural history. In: Weiss EB, Stein M, editors. Bronchial asthma: mechanisms and therapeutics. 3rd ed Little, Brown; Boston: 1993. p. 15.
-
- Fletcher C. The natural history of chronic bronchitis and emphysema: an eight-year study of early chronic obstructive lung disease in working men in London. Oxford University Press; New York: 1976.
-
- Sears MR, Greene JM, Willan AR, et al. A longitudinal, population-based, cohort study of childhood asthma followed to adulthood. N Engl J Med. 2003;349:1414–22. - PubMed
-
- Hospers JJ, Postma DS, Rijcken B, Weiss ST, Schouten JP. Histamine airway hyper-responsiveness and mortality from chronic obstructive pulmonary disease: a cohort study. Lancet. 2000;356:1313–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- P01 HL083069/HL/NHLBI NIH HHS/United States
- K08-HL097029/HL/NHLBI NIH HHS/United States
- R01 HG003143/HG/NHGRI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- K25 HL091124/HL/NHLBI NIH HHS/United States
- K08-HL102265/HL/NHLBI NIH HHS/United States
- U01 HL075408/HL/NHLBI NIH HHS/United States
- R01 HL127200/HL/NHLBI NIH HHS/United States
- T32 HL007427/HL/NHLBI NIH HHS/United States
- K08 HL102265/HL/NHLBI NIH HHS/United States
- R01 HL113264/HL/NHLBI NIH HHS/United States
- U01-HL091075/HL/NHLBI NIH HHS/United States
- R21 HL120794/HL/NHLBI NIH HHS/United States
- HHMI/Howard Hughes Medical Institute/United States
- U01HL075408/HL/NHLBI NIH HHS/United States
- U01 HL105569/HL/NHLBI NIH HHS/United States
- P01-HL105339/HL/NHLBI NIH HHS/United States
- U01 HL091075/HL/NHLBI NIH HHS/United States
- R01-HL124233/HL/NHLBI NIH HHS/United States
- K08 HL097029/HL/NHLBI NIH HHS/United States
- R01-HL113264/HL/NHLBI NIH HHS/United States
- U01 HL065899/HL/NHLBI NIH HHS/United States
- R01HL127200/HL/NHLBI NIH HHS/United States
- R01 HL075478/HL/NHLBI NIH HHS/United States
- T32-HL007427/HL/NHLBI NIH HHS/United States
- U01-HL065899/HL/NHLBI NIH HHS/United States
- R01 NR013391/NR/NINR NIH HHS/United States
- R01-HL089856/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- R33 HL120794/HL/NHLBI NIH HHS/United States
- P01 HL105339/HL/NHLBI NIH HHS/United States
- P01-HL083069/HL/NHLBI NIH HHS/United States
- R21HL120794/HL/NHLBI NIH HHS/United States
- U54 HG007010/HG/NHGRI NIH HHS/United States
- HG007010/HG/NHGRI NIH HHS/United States
- R01 HL124233/HL/NHLBI NIH HHS/United States
- U01-HL105569/HL/NHLBI NIH HHS/United States
- HG003143/HG/NHGRI NIH HHS/United States
- R01-HL075478/HL/NHLBI NIH HHS/United States
- R01-NR013391/NR/NINR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous