

Negative signals for adenomyomatosis of the gallbladder upon diffusion-weighted whole body imaging with background body signal suppression/T2-weighted image fusion analysis
- PMID: 27168802
- PMCID: PMC4840534
- DOI: 10.3892/etm.2016.3126
Negative signals for adenomyomatosis of the gallbladder upon diffusion-weighted whole body imaging with background body signal suppression/T2-weighted image fusion analysis
Abstract
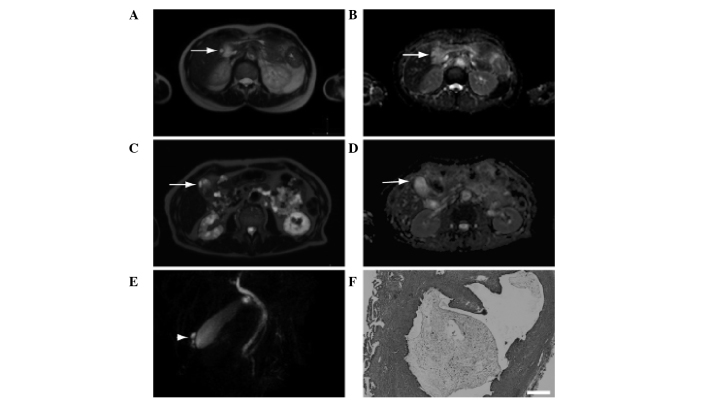
Differentiation between adenomyomatosis (ADM) and cancer of the gallbladder is necessary during diagnosis. Diffusion-weighted whole body imaging with background body signal suppression (DWIBS) images are able to indicate cancer and inflammation. The fusion of a DWIBS with a T2 weighted image (DWIBS/T2) facilitates both functional and anatomical investigations. In the present study, patient records and images from patients with surgically confirmed ADM from April 2012 to October 2014 were analyzed retrospectively. The enrolled patients, including 6 men (64.2±13.1 years) and 4 women (57.3±12.4 years) were subjected to DWIBS/T2 during routine clinical practice. The diagnosis of ADM was based on magnetic resonance cholangiopancreatography, transabdominal ultrasonography, and endoscopic ultrasonography; ADM was diagnosed definitively when cystic lesions were observed, indicating the Rokitansky-Aschoff sinus. A single patient was indicated to be positive by DWIBS/T2 imaging. The Rokitansky-Aschoff sinus revealed a relatively high signal intensity; however, it was not as strong as that of the spleen. The signal intensity was also high on an apparent diffusion coefficient map, suggesting T2 shine-through. The thickened wall displayed low signal intensity. The aforementioned results indicate that ADM may be negative upon DWIBS/T2 imaging; one false positive case was determined to be ADM, accompanied by chronic cholecystitis. The majority of patients with ADM displayed negative findings upon DWIBS/T2 imaging, and chronic cholecystitis may cause false positives.
Keywords: apparent diffusion coefficient; chronic cholecystitis; diffusion weighted imaging; magnetic resonance cholangiopancreatography.
Figures
Similar articles
-
Diffusion-weighted whole-body magnetic resonance imaging with background body signal suppression/T2 image fusion for the diagnosis of acute cholecystitis.Exp Ther Med. 2017 Jul;14(1):730-734. doi: 10.3892/etm.2017.4561. Epub 2017 Jun 8. Exp Ther Med. 2017. PMID: 28672991 Free PMC article.
-
Diagnosis of complications associated with acute cholecystitis using computed tomography and diffusion-weighted imaging with background body signal suppression/T2 image fusion.Exp Ther Med. 2017 Jul;14(1):743-747. doi: 10.3892/etm.2017.4567. Epub 2017 Jun 8. Exp Ther Med. 2017. PMID: 28672993 Free PMC article.
-
Comparison of DWIBS/T2 image fusion and PET/CT for the diagnosis of cancer in the abdominal cavity.Exp Ther Med. 2017 Oct;14(4):3754-3760. doi: 10.3892/etm.2017.4987. Epub 2017 Aug 22. Exp Ther Med. 2017. PMID: 29042975 Free PMC article.
-
A Resected Gallbladder Carcinoma Coexisting With Adenomyomatosis Involving Varied Degrees of Intraepithelial Dysplasia: A Case Report and Literature Review.Surg Laparosc Endosc Percutan Tech. 2019 Aug;29(4):290-296. doi: 10.1097/SLE.0000000000000617. Surg Laparosc Endosc Percutan Tech. 2019. PMID: 30570538 Review.
-
Gallbladder adenomyomatosis: Diagnosis and management.J Visc Surg. 2017 Oct;154(5):345-353. doi: 10.1016/j.jviscsurg.2017.06.004. Epub 2017 Aug 24. J Visc Surg. 2017. PMID: 28844704 Review.
Cited by
-
Gallbladder Adenomyomatosis Mimicking Carcinoma: A Diagnostic Dilemma.J Glob Oncol. 2016 Jun 15;2(5):341-345. doi: 10.1200/JGO.2016.005249. eCollection 2016 Oct. J Glob Oncol. 2016. PMID: 28717718 Free PMC article. No abstract available.
-
The Influence of Bowel Preparation on ADC Measurements: Comparison between Conventional DWI and DWIBS Sequences.Medicina (Kaunas). 2019 Jul 21;55(7):394. doi: 10.3390/medicina55070394. Medicina (Kaunas). 2019. PMID: 31330916 Free PMC article.
References
-
- Kim JH, Jeong IH, Han JH, Kim JH, Hwang JC, Yoo BM, Kim JH, Kim MW, Kim WH. Clinical/pathological analysis of gallbladder adenomyomatosis; Type and pathogenesis. Hepatogastroenterology. 2010;57:420–425. - PubMed
-
- Kim BS, Oh JY, Nam KJ, Cho JH, Kwon HJ, Yoon SK, Jeong JS, Noh MH. Focal thickening at the fundus of the gallbladder: Computed tomography differentiation of fundal type adenomyomatosis and localized chronic cholecystitis. Gut Liver. 2014;8:219–223. doi: 10.5009/gnl.2014.8.2.219. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous