

Effect of a mixed reality-based intervention on arm, hand, and finger function on chronic stroke
- PMID: 27169462
- PMCID: PMC4864937
- DOI: 10.1186/s12984-016-0153-6
Effect of a mixed reality-based intervention on arm, hand, and finger function on chronic stroke
Erratum in
-
Erratum to: Effect of a mixed reality-based intervention on arm, hand, and finger function on chronic stroke.J Neuroeng Rehabil. 2017 Feb 14;14(1):12. doi: 10.1186/s12984-017-0224-3. J Neuroeng Rehabil. 2017. PMID: 28196508 Free PMC article. No abstract available.
Abstract
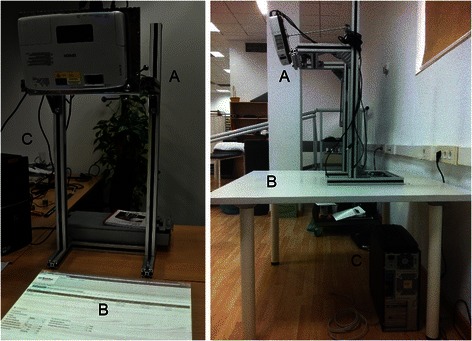
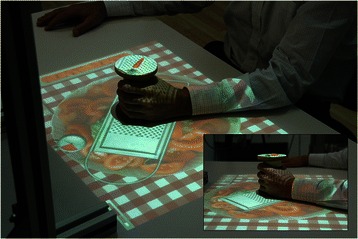
Background: Virtual and mixed reality systems have been suggested to promote motor recovery after stroke. Basing on the existing evidence on motor learning, we have developed a portable and low-cost mixed reality tabletop system that transforms a conventional table in a virtual environment for upper limb rehabilitation. The system allows intensive and customized training of a wide range of arm, hand, and finger movements and enables interaction with tangible objects, while providing audiovisual feedback of the participants' performance in gamified tasks. This study evaluates the clinical effectiveness and the acceptance of an experimental intervention with the system in chronic stroke survivors.
Methods: Thirty individuals with stroke were included in a reversal (A-B-A) study. Phase A consisted of 30 sessions of conventional physical therapy. Phase B consisted of 30 training sessions with the experimental system. Both interventions involved flexion and extension of the elbow, wrist, and fingers, and grasping of different objects. Sessions were 45-min long and were administered three to five days a week. The body structures (Modified Ashworth Scale), functions (Motricity Index, Fugl-Meyer Assessment Scale), activities (Manual Function Test, Wolf Motor Function Test, Box and Blocks Test, Nine Hole Peg Test), and participation (Motor Activity Log) were assessed before and after each phase. Acceptance of the system was also assessed after phase B (System Usability Scale, Intrinsic Motivation Inventory).
Results: Significant improvement was detected after the intervention with the system in the activity, both in arm function measured by the Wolf Motor Function Test (p < 0.01) and finger dexterity measured by the Box and Blocks Test (p < 0.01) and the Nine Hole Peg Test (p < 0.01); and participation (p < 0.01), which was maintained to the end of the study. The experimental system was reported as highly usable, enjoyable, and motivating.
Conclusions: Our results support the clinical effectiveness of mixed reality interventions that satisfy the motor learning principles for upper limb rehabilitation in chronic stroke survivors. This characteristic, together with the low cost of the system, its portability, and its acceptance could promote the integration of these systems in the clinical practice as an alternative to more expensive systems, such as robotic instruments.
Keywords: Augmented reality; Hemiparesis; Physical therapy; Stroke; Tabletop systems; Upper limb; Virtual reality.
Figures


Similar articles
-
Effects of electromyography-driven robot-aided hand training with neuromuscular electrical stimulation on hand control performance after chronic stroke.Disabil Rehabil Assist Technol. 2015 Mar;10(2):149-59. doi: 10.3109/17483107.2013.873491. Epub 2013 Dec 31. Disabil Rehabil Assist Technol. 2015. PMID: 24377757
-
Motor skill changes and neurophysiologic adaptation to recovery-oriented virtual rehabilitation of hand function in a person with subacute stroke: a case study.Disabil Rehabil. 2017 Jul;39(15):1524-1531. doi: 10.1080/09638288.2016.1226421. Epub 2016 Sep 27. Disabil Rehabil. 2017. PMID: 27669997 Free PMC article.
-
Effectiveness of mixed reality-based rehabilitation on hands and fingers by individual finger-movement tracking in patients with stroke.J Neuroeng Rehabil. 2024 Aug 10;21(1):140. doi: 10.1186/s12984-024-01418-6. J Neuroeng Rehabil. 2024. PMID: 39127667 Free PMC article.
-
Effect of Traditional Plus Virtual Reality Rehabilitation on Prognosis of Stroke Survivors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Am J Phys Med Rehabil. 2022 Mar 1;101(3):217-228. doi: 10.1097/PHM.0000000000001775. Am J Phys Med Rehabil. 2022. PMID: 33929347
-
Exoskeleton versus end-effector robot-assisted therapy for finger-hand motor recovery in stroke survivors: systematic review and meta-analysis.Top Stroke Rehabil. 2022 Dec;29(8):539-550. doi: 10.1080/10749357.2021.1967657. Epub 2021 Aug 21. Top Stroke Rehabil. 2022. PMID: 34420498
Cited by
-
ARMIA: A Sensorized Arm Wearable for Motor Rehabilitation.Biosensors (Basel). 2022 Jun 29;12(7):469. doi: 10.3390/bios12070469. Biosensors (Basel). 2022. PMID: 35884272 Free PMC article.
-
Effect of Virtual Reality-Based Therapies on Lower Limb Functional Recovery in Stroke Survivors: Systematic Review and Meta-Analysis.J Med Internet Res. 2025 Jul 30;27:e72364. doi: 10.2196/72364. J Med Internet Res. 2025. PMID: 40737641 Free PMC article.
-
Reliability and Validity of the Motor Activity Log (MAL-30) Scale for Post-Stroke Patients in a Spanish Sample.Int J Environ Res Public Health. 2022 Nov 14;19(22):14964. doi: 10.3390/ijerph192214964. Int J Environ Res Public Health. 2022. PMID: 36429681 Free PMC article.
-
A Taxonomy for Augmented and Mixed Reality Applications to Support Physical Exercises in Medical Rehabilitation-A Literature Review.Healthcare (Basel). 2022 Mar 30;10(4):646. doi: 10.3390/healthcare10040646. Healthcare (Basel). 2022. PMID: 35455824 Free PMC article. Review.
-
Brazilian practice guidelines for stroke rehabilitation: Part II.Arq Neuropsiquiatr. 2022 Jul;80(7):741-758. doi: 10.1055/s-0042-1757692. Epub 2022 Sep 29. Arq Neuropsiquiatr. 2022. PMID: 36254447 Free PMC article.
References
-
- Kwakkel G, Kollen B, Lindeman E. Understanding the pattern of functional recovery after stroke: facts and theories. Restor Neurol Neurosci. 2004;22(3–5):281–99. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
