

Cellular mechanisms of skin repair in humans and other mammals
- PMID: 27170326
- PMCID: PMC4882309
- DOI: 10.1007/s12079-016-0330-1
Cellular mechanisms of skin repair in humans and other mammals
Abstract
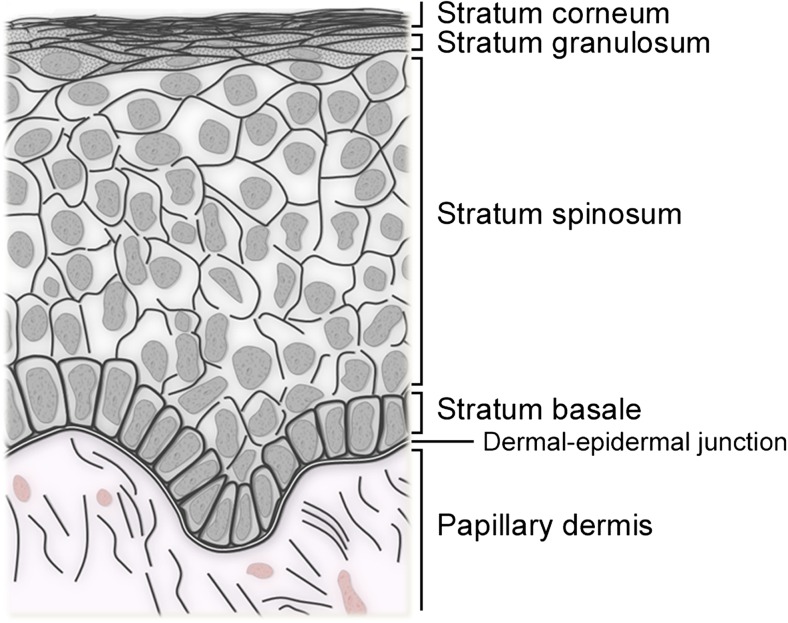
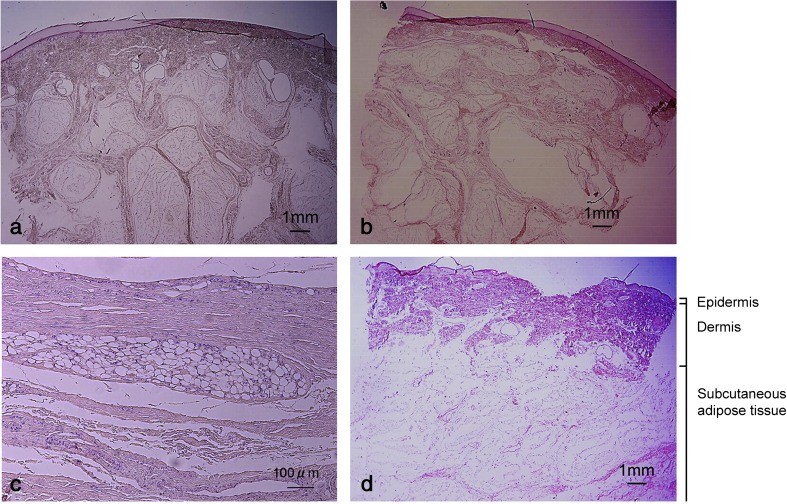
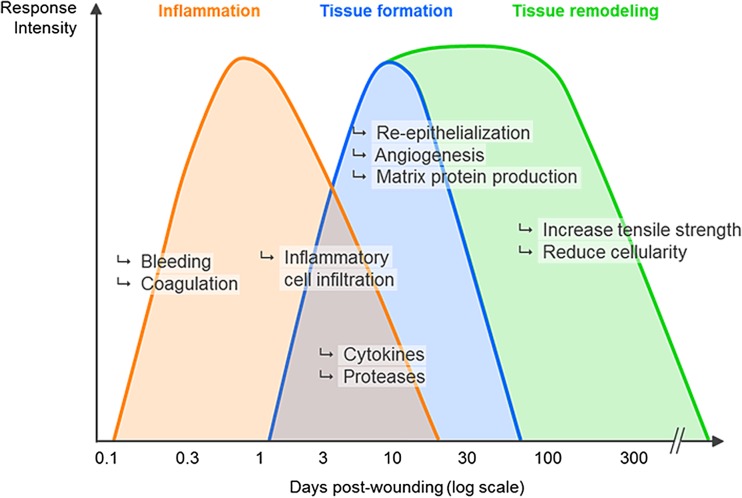
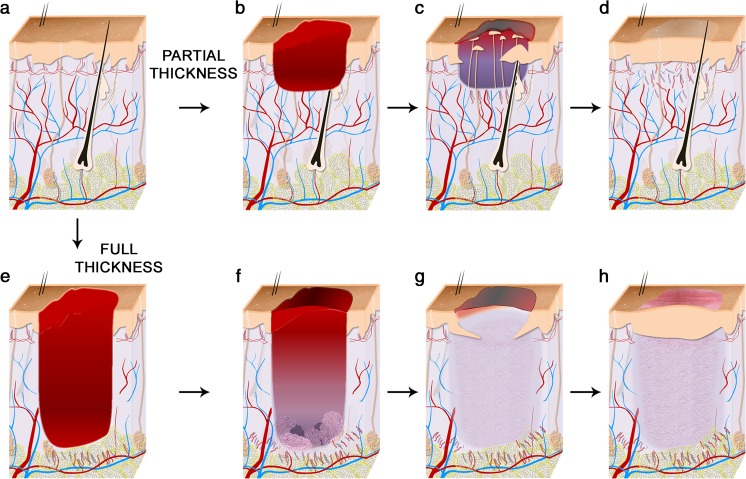
The increased incidence of non-healing skin wounds in developed societies has prompted tremendous research efforts on the complex process known as "wound healing". Unfortunately, the weak relevance of modern wound healing research to human health continues to be a matter of concern. This review summarizes the current knowledge of the cellular mechanisms that mediate wound closure in the skin of humans and laboratory animals. The author highlights the anatomical singularities of human skin vs. the skin of other mammals commonly used for wound healing research (i.e. as mice, rats, rabbits, and pigs), and discusses the roles of stem cells, myofibroblasts, and the matrix environment in the repair process. The majority of this review focuses on reepithelialization and wound closure. Other aspects of wound healing (e.g. inflammation, fibrous healing) are referred to when relevant to the main topic. This review aims at providing the reader with a clear understanding of the similarities and differences that have been reported over the past 100 years between the healing of human wounds and that of other mammals.
Keywords: Epidermis; Extracellular matrix; Granulation tissue; Mechanical force; Myofibroblast; Skin; Stem cells; Wound healing.
Figures
References
-
- Arey LB. Certain basic principles of wound healing. Anat Rec. 1932;51:299–313. doi: 10.1002/ar.1090510309. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
