

Effects of the Alternate Combination of "Error-Enhancing" and "Active Assistive" Robot-Mediated Treatments on Stroke Patients
- PMID: 27170850
- PMCID: PMC4819227
- DOI: 10.1109/JTEHM.2013.2271898
Effects of the Alternate Combination of "Error-Enhancing" and "Active Assistive" Robot-Mediated Treatments on Stroke Patients
Abstract
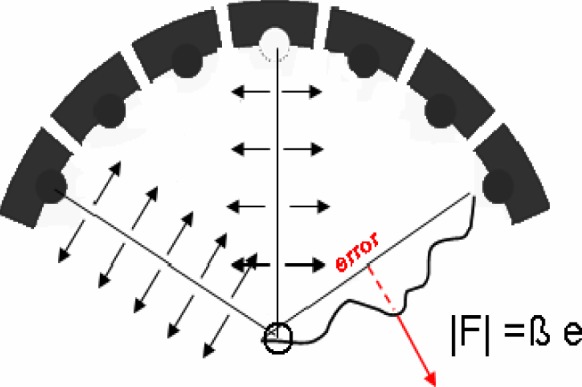
This paper aimed at investigating the effects of a novel robotic-aided rehabilitation treatment for the recovery of the upper limb related capabilities in chronic post stroke patients. Eighteen post-stroke patients were enrolled in a six-week therapy program and divided into two groups. They were all required to perform horizontal pointing movements both in the presence of a robot-generated divergent force field (DF) that pushed their hands proportional to the trajectory error and perpendicular to the direction of motion, and according to the typical active assistive (AA) approach used in robotic therapy. We used a crossover experimental paradigm where the two groups switched from one therapy treatment to the other. The hypothesis underlying this paper was that the use of the destabilizing scenario forced the patient to keep the end-point position as close as possible to the ideal path, hence requiring a more active control of the arm with respect to the AA approach. Our findings confirmed this hypothesis. In addition, when the DF treatment was provided in the first therapy cycle, patients also showed straighter and smoother paths during the subsequent AA therapy cycle, while this was not true in the opposite case. In conclusion, the results herein reported provide evidence that the use of an unstable DF field can lead to better recovery outcomes, and therefore it potentially more effective than solely active assistance therapy alone.
Keywords: Rehabilitation robotics; assisted-as-needed; error-enhancing; stroke; upper arm.
Figures




References
-
- Fasoli S. E., Krebs H. I., Stein J., Frontera W. R., and Hogan N., “Effects of robotic therapy on motor impairment and recovery in chronic stroke,” in Archives Phys. Med. Rehabil., vol. 84, no. 4, pp. 477–482, Apr. 2003. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
