

Socioeconomic Inequalities in Neglected Tropical Diseases: A Systematic Review
- PMID: 27171166
- PMCID: PMC4865383
- DOI: 10.1371/journal.pntd.0004546
Socioeconomic Inequalities in Neglected Tropical Diseases: A Systematic Review
Abstract
Background: Neglected tropical diseases (NTDs) are generally assumed to be concentrated in poor populations, but evidence on this remains scattered. We describe within-country socioeconomic inequalities in nine NTDs listed in the London Declaration for intensified control and/or elimination: lymphatic filariasis (LF), onchocerciasis, schistosomiasis, soil-transmitted helminthiasis (STH), trachoma, Chagas' disease, human African trypanosomiasis (HAT), leprosy, and visceral leishmaniasis (VL).
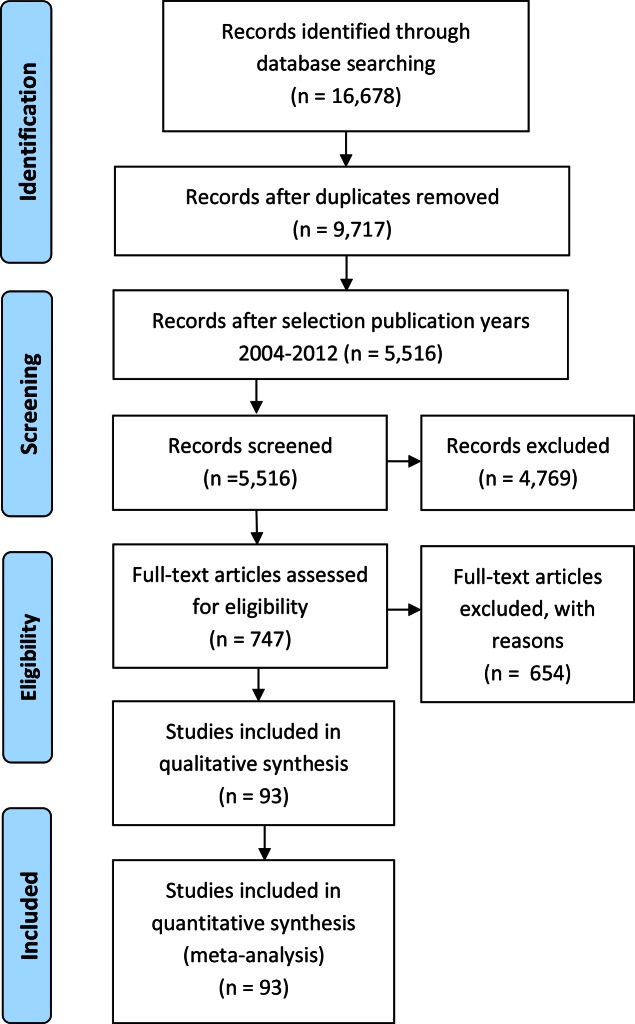
Methodology: We conducted a systematic literature review, including publications between 2004-2013 found in Embase, Medline (OvidSP), Cochrane Central, Web of Science, Popline, Lilacs, and Scielo. We included publications in international peer-reviewed journals on studies concerning the top 20 countries in terms of the burden of the NTD under study.
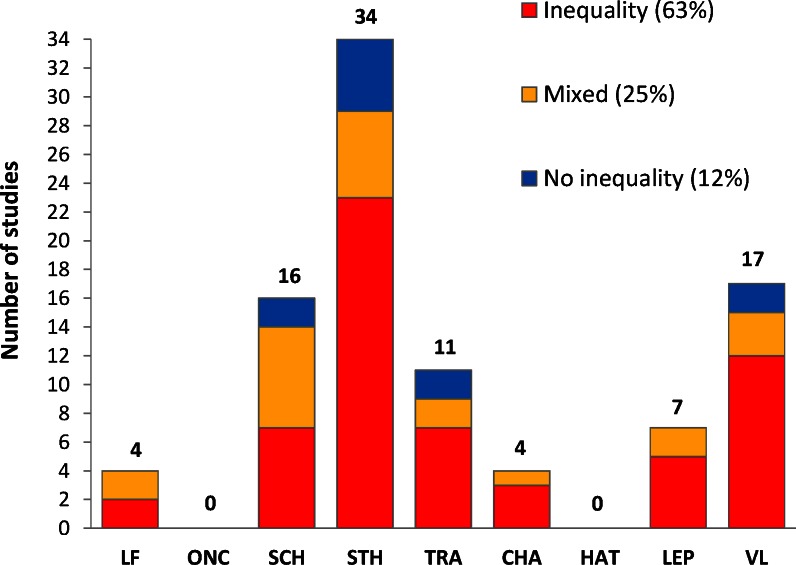
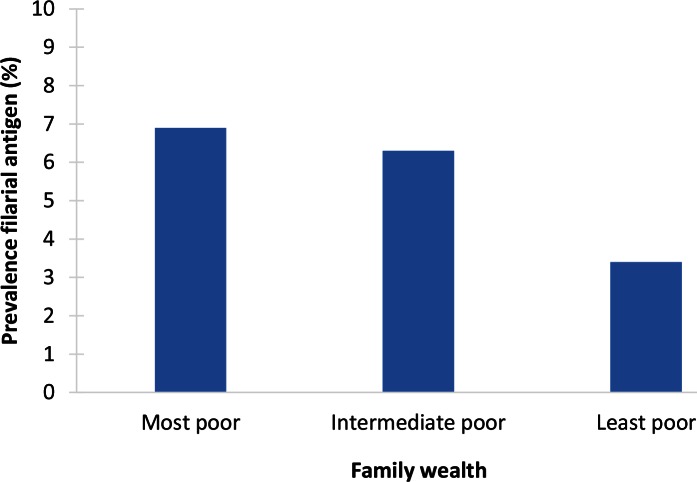
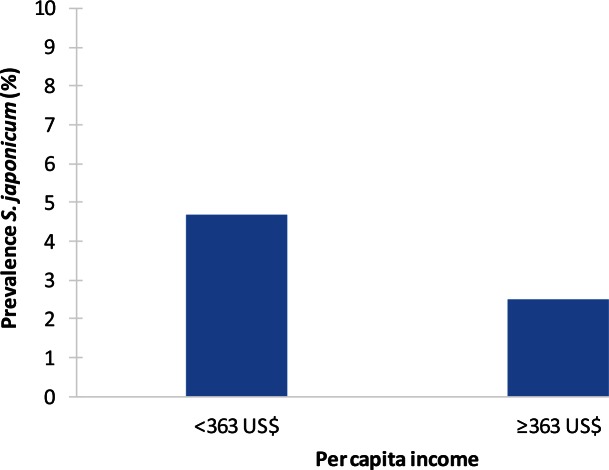
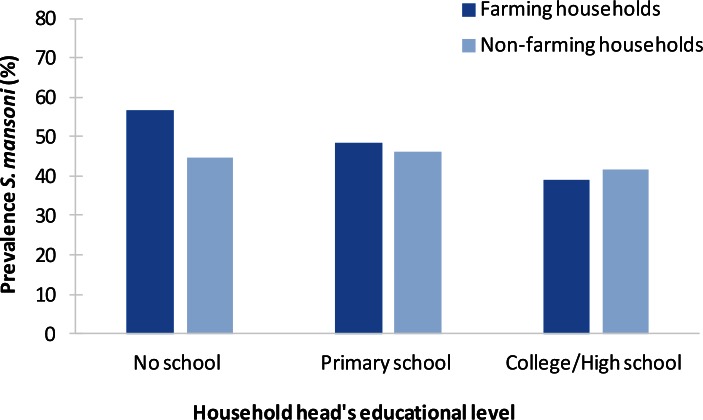
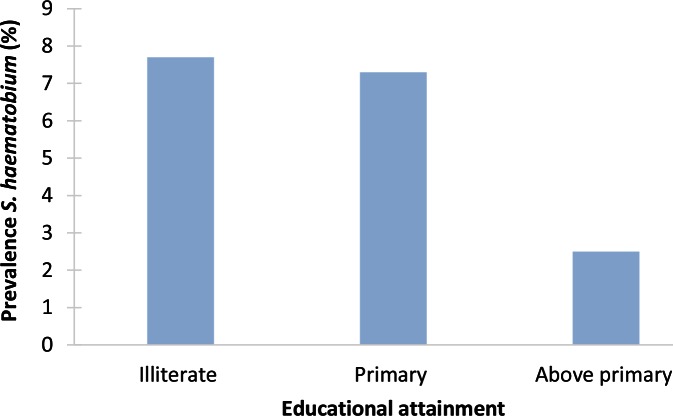
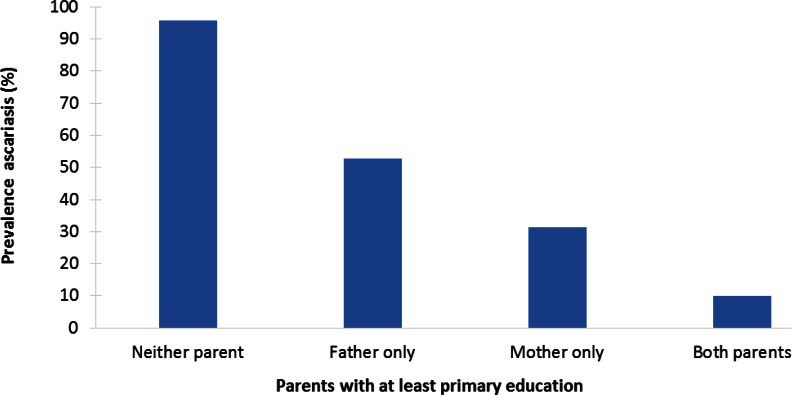
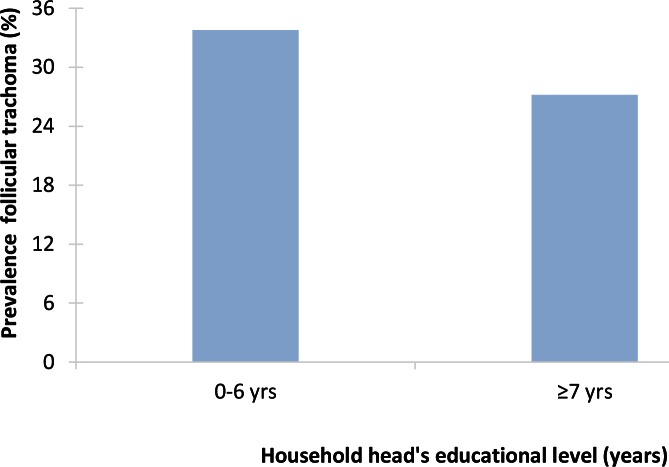
Principal findings: We identified 5,516 publications, of which 93 met the inclusion criteria. Of these, 59 papers reported substantial and statistically significant socioeconomic inequalities in NTD distribution, with higher odds of infection or disease among poor and less-educated people compared with better-off groups. The findings were mixed in 23 studies, and 11 studies showed no substantial or statistically significant inequality. Most information was available for STH, VL, schistosomiasis, and, to a lesser extent, for trachoma. For the other NTDs, evidence on their socioeconomic distribution was scarce. The magnitude of inequality varied, but often, the odds of infection or disease were twice as high among socioeconomically disadvantaged groups compared with better-off strata. Inequalities often took the form of a gradient, with higher odds of infection or disease each step down the socioeconomic hierarchy. Notwithstanding these inequalities, the prevalence of some NTDs was sometimes also high among better-off groups in some highly endemic areas.
Conclusions: While recent evidence on socioeconomic inequalities is scarce for most individual NTDs, for some, there is considerable evidence of substantially higher odds of infection or disease among socioeconomically disadvantaged groups. NTD control activities as proposed in the London Declaration, when set up in a way that they reach the most in need, will benefit the poorest populations in poor countries.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Hotez PJ. The Disease Next Door. Foreign Policy. 2013;March 25.
-
- Aagaard-Hansen J, Chaignat CL. Neglected tropical diseases: equity and social determinants In: Blas E, Sivasankara Kurup A, editors. Equity, social determinants and public health programmes Geneva: World Health Organization; 2010. p. 135–57.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
