

Predictors for Delayed Emergency Department Care in Medical Patients with Acute Infections - An International Prospective Observational Study
- PMID: 27171476
- PMCID: PMC4865227
- DOI: 10.1371/journal.pone.0155363
Predictors for Delayed Emergency Department Care in Medical Patients with Acute Infections - An International Prospective Observational Study
Abstract
Introduction: In overcrowded emergency department (ED) care, short time to start effective antibiotic treatment has been evidenced to improve infection-related clinical outcomes. Our objective was to study factors associated with delays in initial ED care within an international prospective medical ED patient population presenting with acute infections.
Methods: We report data from an international prospective observational cohort study including patients with a main diagnosis of infection from three tertiary care hospitals in Switzerland, France and the United States (US). We studied predictors for delays in starting antibiotic treatment by using multivariate regression analyses.
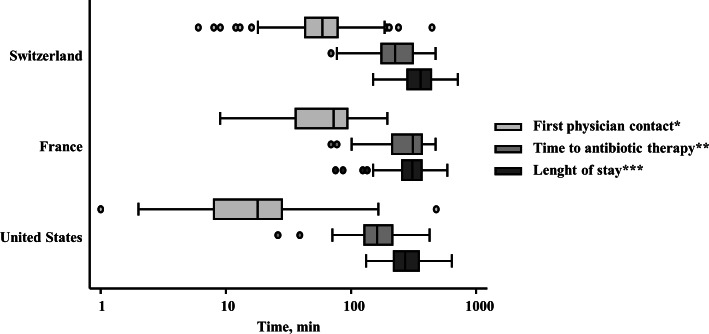
Results: Overall, 544 medical ED patients with a main diagnosis of acute infection and antibiotic treatment were included, mainly pneumonia (n = 218; 40.1%), urinary tract (n = 141; 25.9%), and gastrointestinal infections (n = 58; 10.7%). The overall median time to start antibiotic therapy was 214 minutes (95% CI: 199, 228), with a median length of ED stay (ED LOS) of 322 minutes (95% CI: 308, 335). We found large variations of time to start antibiotic treatment depending on hospital centre and type of infection. The diagnosis of a gastrointestinal infection was the most significant predictor for delay in antibiotic treatment (+119 minutes compared to patients with pneumonia; 95% CI: 58, 181; p<0.001).
Conclusions: We found high variations in hospital ED performance in regard to start antibiotic treatment. The implementation of measures to reduce treatment times has the potential to improve patient care.
Conflict of interest statement
Figures
Similar articles
-
Procalcitonin variations after Emergency Department admission are highly predictive of hospital mortality in patients with acute infectious diseases.Eur Rev Med Pharmacol Sci. 2013 Feb;17 Suppl 1:133-42. Eur Rev Med Pharmacol Sci. 2013. PMID: 23436675
-
Epidemiology, recognition and documentation of sepsis in the pre-hospital setting and associated clinical outcomes: a prospective multicenter study.Acute Med. 2016;15(4):168-175. Acute Med. 2016. PMID: 28112285
-
ED antibiotic use for acute respiratory illnesses since pneumonia performance measure inception.Am J Emerg Med. 2010 Jan;28(1):23-31. doi: 10.1016/j.ajem.2008.09.023. Am J Emerg Med. 2010. PMID: 20006197 Clinical Trial.
-
International perspectives on emergency department crowding.Acad Emerg Med. 2011 Dec;18(12):1358-70. doi: 10.1111/j.1553-2712.2011.01235.x. Acad Emerg Med. 2011. PMID: 22168200 Review.
-
The role of new antibiotics for the treatment of infections in the emergency department.Ann Emerg Med. 1994 Sep;24(3):473-89. doi: 10.1016/s0196-0644(94)70186-5. Ann Emerg Med. 1994. PMID: 8080145 Review.
Cited by
-
CD169 and CD64 could help differentiate bacterial from CoVID-19 or other viral infections in the Emergency Department.Cytometry A. 2021 May;99(5):435-445. doi: 10.1002/cyto.a.24314. Epub 2021 Feb 8. Cytometry A. 2021. PMID: 33491921 Free PMC article.
-
Assessment of factors that influence timely administration of initial antibiotic dose using collaborative process mapping at a referral hospital in Malawi: a case study of pneumonia patients.BMC Infect Dis. 2018 Dec 27;18(1):697. doi: 10.1186/s12879-018-3620-9. BMC Infect Dis. 2018. PMID: 30587155 Free PMC article.
-
Comparative quality measures of emergency care: an outcome cockpit proposal to survey clinical processes in real life.Open Access Emerg Med. 2017 Oct 24;9:97-106. doi: 10.2147/OAEM.S145342. eCollection 2017. Open Access Emerg Med. 2017. PMID: 29123431 Free PMC article.
-
Organizational Benefits of Ultra-Low-Dose Chest CT Compared to Chest Radiography in the Emergency Department for the Diagnostic Workup of Community-Acquired Pneumonia: A Real-Life Retrospective Analysis.Medicina (Kaunas). 2023 Aug 22;59(9):1508. doi: 10.3390/medicina59091508. Medicina (Kaunas). 2023. PMID: 37763627 Free PMC article.
-
Length of Stay in the Emergency Department and Its Associated Factors at Jimma Medical Center, Southwest Ethiopia.Open Access Emerg Med. 2020 Oct 9;12:227-235. doi: 10.2147/OAEM.S254239. eCollection 2020. Open Access Emerg Med. 2020. PMID: 33116958 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
