

Association of time since pneumococcal polysaccharide vaccine receipt and CD4 count with antibody response to the 13-valent pneumococcal conjugate vaccine in HIV-infected adults
- PMID: 27172241
- PMCID: PMC4994738
- DOI: 10.1080/21645515.2016.1160987
Association of time since pneumococcal polysaccharide vaccine receipt and CD4 count with antibody response to the 13-valent pneumococcal conjugate vaccine in HIV-infected adults
Abstract
Introduction: Pneumococcal infection is a leading cause of illness and death in HIV-infected adults. Current United States guidelines for HIV-infected adults recommend a single dose of the 13-valent pneumococcal conjugate vaccine (PCV-13) at any CD4 count and at least 1 y after receipt of the 23-valent pneumococcal polysaccharide vaccine (PPV). PPV is known to lead to hyporesponsiveness to subsequent pneumococcal vaccines for at least 1 y Whether PCV-13 would be more immunogenic if administered later after PPV receipt or at higher CD4 counts has not been tested.
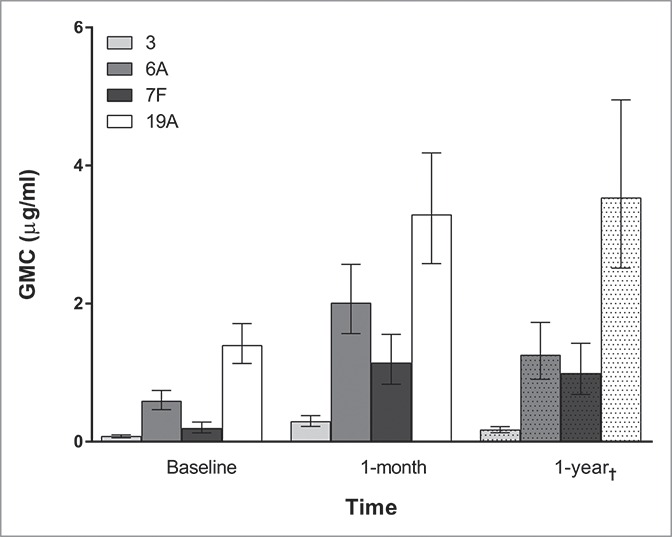
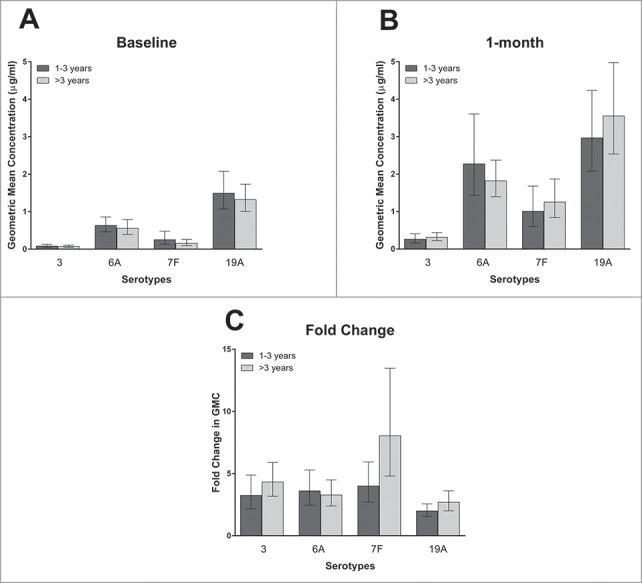
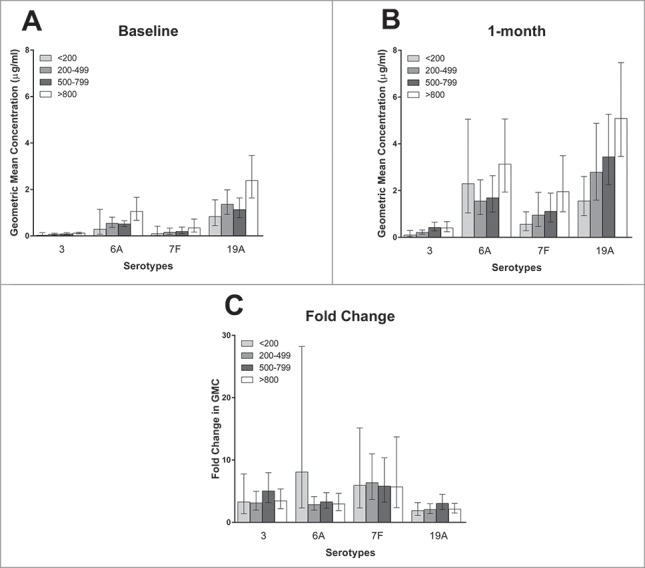
Methods: We prospectively collected serum from 96 HIV-infected adults before and after PCV-13 receipt, and measured antibody concentrations against 4 pneumococcal serotypes (3, 6A, 7F, and 19A) via indirect ELISA according to the WHO protocol. Post-booster antibody concentrations and fold-rise in antibody concentrations were compared according to time from PPV receipt and baseline CD4 count using univariate and multivariate analyses.
Results: PPV receipt >3 versus 1-3 y prior did not significantly change post-vaccination antibody concentrations, but was associated with slightly higher fold-rise in antibody concentration for the 3 tested serotypes included in PPV, though this only reached significance for serotype 7F. CD4 count was significantly associated with post-vaccination antibody concentrations for 3 of 4 serotypes, but not for fold-rise in antibody concentration for any serotype.
Conclusion: Waiting longer than 1 y after PPV receipt to administer PCV-13 may slightly improve the antibody response to serotypes included in both vaccines. While higher CD4 count at PCV-13 administration results in higher post-vaccination antibody concentrations, this is likely because higher CD4 count is also associated with higher pre-vaccination antibody concentrations.
Keywords: CD4 Count; HIV; Pneumovax; Prevnar; adults; pneumococcus; vaccine.
Figures
References
-
- Heffernan RT, Barrett NL, Gallagher KM, Hadler JL, Harrison LH, Reingold AL, Khoshnood K, Holford TR, Schuchat A. Declining incidence of invasive Streptococcus pneumoniae infections among persons with AIDS in an era of highly active antiretroviral therapy, 1995–2000. J Infect Dis 2005; 191:2038-45; PMID:15897989; http://dx.doi.org/10.1086/430356 - DOI - PubMed
-
- French N, Gordon SB, Mwalukomo T, White SA, Mwafulirwa G, Longwe H, Mwaiponya M, Zijlstra EE, Molyneux ME, Gilks CF. A trial of a 7-valent pneumococcal conjugate vaccine in HIV-infected adults. N Engl J Med 2010; 362:812-22; PMID:20200385; http://dx.doi.org/10.1056/NEJMoa0903029 - DOI - PMC - PubMed
-
- Info.NIH A Guidelines for the Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents. 2015
-
- (CDC) CfDCaP . Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2012; 61:816-9; PMID:23051612 - PubMed
-
- Bonten MJ, Huijts SM, Bolkenbaas M, Webber C, Patterson S, Gault S, van Werkhoven CH, van Deursen AM, Sanders EA, Verheij TJ, et al.. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N Engl J Med 2015; 372:1114-25; PMID:25785969; http://dx.doi.org/10.1056/NEJMoa1408544 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials