

Nationwide trends of hospital admissions for acute cholecystitis in the United States
- PMID: 27174434
- PMCID: PMC5444253
- DOI: 10.1093/gastro/gow015
Nationwide trends of hospital admissions for acute cholecystitis in the United States
Abstract
Background and aims: Acute cholecystitis is a fairly common inpatient diagnosis among the gastrointestinal disorders. The aim of this study was to use a national database of US hospitals to evaluate the incidence and costs of hospital admissions associated with acute cholecystitis.
Method: We analyzed the National Inpatient Sample Database (NIS) for all patients in which acute cholecystitis (ICD-9 codes: 574.00, 574.01, 574.30, 574.31, 574.60, 574.61 or 575.0) was the principal discharge diagnosis from 1997 to 2012. The NIS is the largest all-payer inpatient database in the United States and contains data from approximately 8 million hospital stays each year. The statistical significance of the difference in the number of hospital discharges, lengths of stay and associated hospital costs over the study period was determined by using the Chi-square test for trends.
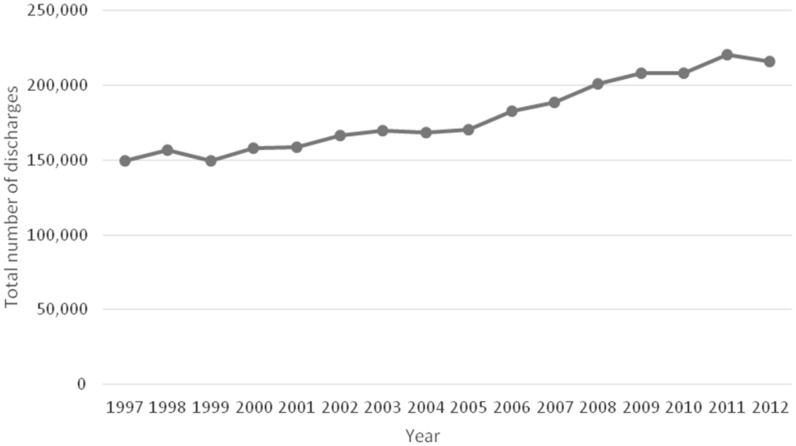
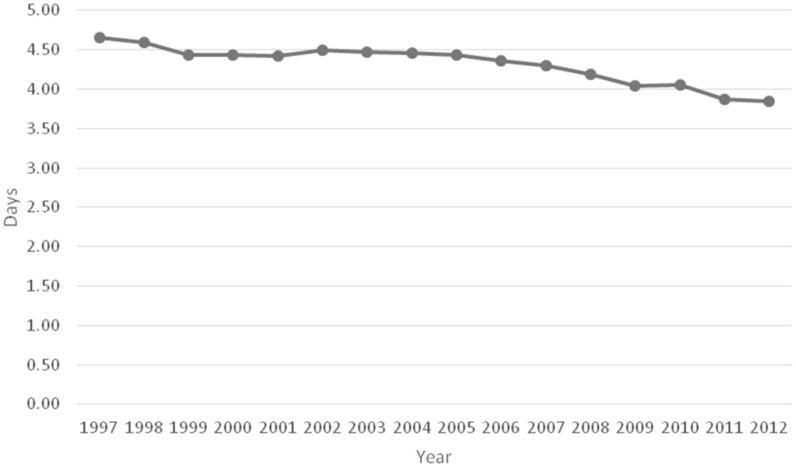
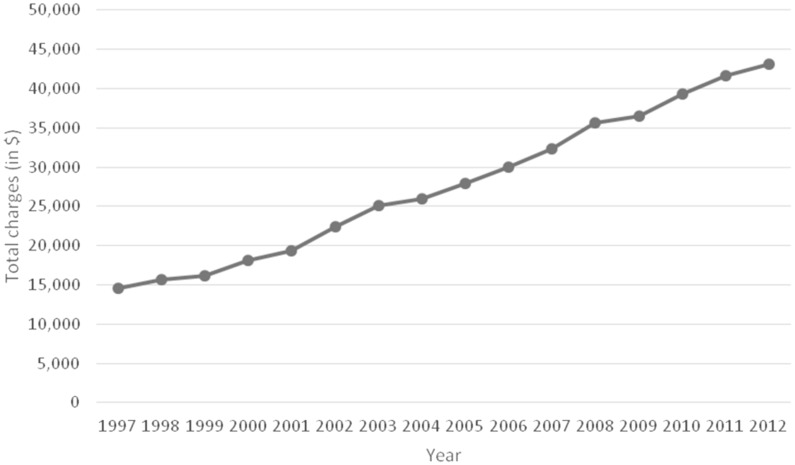
Results: In 1997, there were 149 661 hospital admissions with a principal discharge diagnosis of acute cholecystitis, which increased to 215 995 in 2012 ( P < 0.001). The mean length of stay for acute cholecystitis decreased by 17% between 1997 and 2012 (i.e. from 4.7 days to 3.9 days; (P < 0.05). During the same time period, however, mean hospital charges have increased by 195.4 % from US$14 608 per patient in 1997 to US$43 152 per patient in 2012 ( P < 0.001).
Conclusion: The number of inpatient discharges related to acute cholecystitis has increased significantly in the United States over the last 16 years, along with a great increase in the associated hospital charges. However, there has been a gradual decline in the mean length of stay. Inpatient costs associated with acute cholecystitis contribute significantly to the total healthcare bill. Further research on cost-effective evaluation and management of acute cholecystitis is required.
Keywords: acute cholecystitis; epidemiology; inpatient admission rates; trends.
© The Author(s) 2016. Published by Oxford University Press and Sixth Affiliated Hospital of Sun Yat-Sen University.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
