

Monro-Kellie 2.0: The dynamic vascular and venous pathophysiological components of intracranial pressure
- PMID: 27174995
- PMCID: PMC4971608
- DOI: 10.1177/0271678X16648711
Monro-Kellie 2.0: The dynamic vascular and venous pathophysiological components of intracranial pressure
Abstract
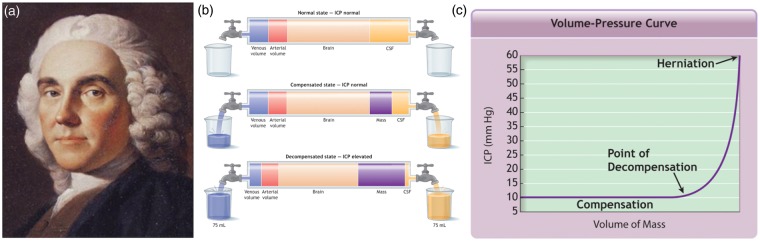
For 200 years, the 'closed box' analogy of intracranial pressure (ICP) has underpinned neurosurgery and neuro-critical care. Cushing conceptualised the Monro-Kellie doctrine stating that a change in blood, brain or CSF volume resulted in reciprocal changes in one or both of the other two. When not possible, attempts to increase a volume further increase ICP. On this doctrine's "truth or relative untruth" depends many of the critical procedures in the surgery of the central nervous system. However, each volume component may not deserve the equal weighting this static concept implies. The slow production of CSF (0.35 ml/min) is dwarfed by the dynamic blood in and outflow (∼700 ml/min). Neuro-critical care practice focusing on arterial and ICP regulation has been questioned. Failure of venous efferent flow to precisely match arterial afferent flow will yield immediate and dramatic changes in intracranial blood volume and pressure. Interpreting ICP without interrogating its core drivers may be misleading. Multiple clinical conditions and the cerebral effects of altitude and microgravity relate to imbalances in this dynamic rather than ICP per se. This article reviews the Monro-Kellie doctrine, categorises venous outflow limitation conditions, relates physiological mechanisms to clinical conditions and suggests specific management options.
Keywords: Intracranial pressure; Monro-Kellie; cerebral venous outflow; intracranial hypertension; neurotrauma.
© The Author(s) 2016.
Figures
Similar articles
-
Continuous monitoring of the Monro-Kellie doctrine: is it possible?J Neurotrauma. 2012 May 1;29(7):1354-63. doi: 10.1089/neu.2011.2018. Epub 2011 Nov 4. J Neurotrauma. 2012. PMID: 21895518 Free PMC article.
-
The cerebral venous system and hypoxia.J Appl Physiol (1985). 2016 Jan 15;120(2):244-50. doi: 10.1152/japplphysiol.00327.2015. Epub 2015 Aug 20. J Appl Physiol (1985). 2016. PMID: 26294747 Review.
-
ICP and CBF regulation: a new hypothesis to explain the "windkessel" phenomenon.Acta Neurochir Suppl. 2002;81:112-6. Acta Neurochir Suppl. 2002. PMID: 12168279
-
Monro-Kellie 4.0: moving from intracranial pressure to intracranial dynamics.Crit Care. 2025 Jun 5;29(1):229. doi: 10.1186/s13054-025-05476-7. Crit Care. 2025. PMID: 40474297 Free PMC article. Review.
-
The new ICP minimally invasive method shows that the Monro-Kellie doctrine is not valid.Acta Neurochir Suppl. 2012;114:117-20. doi: 10.1007/978-3-7091-0956-4_21. Acta Neurochir Suppl. 2012. PMID: 22327675
Cited by
-
Editorial: Cerebrospinal fluid dynamics and intracranial pressure elevation-Novel insights on molecular and physiological mechanisms, and implications for neurological disease.Front Mol Neurosci. 2022 Dec 28;15:1119980. doi: 10.3389/fnmol.2022.1119980. eCollection 2022. Front Mol Neurosci. 2022. PMID: 36644618 Free PMC article. No abstract available.
-
Non-Invasive Spectroscopy for Measuring Cerebral Tissue Oxygenation and Metabolism as a Function of Cerebral Perfusion Pressure.Metabolites. 2022 Jul 20;12(7):667. doi: 10.3390/metabo12070667. Metabolites. 2022. PMID: 35888791 Free PMC article.
-
An update to the Monro-Kellie doctrine to reflect tissue compliance after severe ischemic and hemorrhagic stroke.Sci Rep. 2020 Dec 16;10(1):22013. doi: 10.1038/s41598-020-78880-4. Sci Rep. 2020. PMID: 33328490 Free PMC article.
-
Evolving concepts in intracranial pressure monitoring - from traditional monitoring to precision medicine.Neurotherapeutics. 2025 Jan;22(1):e00507. doi: 10.1016/j.neurot.2024.e00507. Epub 2025 Jan 3. Neurotherapeutics. 2025. PMID: 39753383 Free PMC article. Review.
-
Tentorial Venous Anatomy: Cadaveric and Radiographic Study with Discussion of Origin and Surgical Significance.World Neurosurg. 2019 Nov;131:e38-e45. doi: 10.1016/j.wneu.2019.06.232. Epub 2019 Jul 9. World Neurosurg. 2019. PMID: 31295599 Free PMC article.
References
-
- Restak R. Fixing the brain. Mysteries of the mind, Washington, DC: National Geographic Society, 2000.
-
- Monro A. Observations on the structure and function of the nervous system, Edinburgh: Creech and Johnson, 1783.
-
- Kellie G. An account of the appearances observed in the dissection of two of the three individuals presumed to have perished in the storm of the 3rd, and whose bodies were discovered in the vicinity of Leith on the morning of the 4th November 1821 with some reflections on the pathology of the brain. Transac Medico Chirurg Soc Edinburgh 1824; 1: 84–169. - PMC - PubMed
-
- Clarke C, Abercrombie J. Pathological and practical researches in disease of the brain and spinal cord, Edinburgh: Carey, Lea and Blanchard, 1928.
-
- Magendie F. Recherches anatomique et physiologique sur le liquide céphalo-rachidien ou cérebro-spinal, Paris: Méquignon-Marvis fils, 1842.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
