

Comparison of benefit-risk preferences of patients and physicians regarding cyclooxygenase-2 inhibitors using discrete choice experiments
- PMID: 27175064
- PMCID: PMC4854248
- DOI: 10.2147/PPA.S98228
Comparison of benefit-risk preferences of patients and physicians regarding cyclooxygenase-2 inhibitors using discrete choice experiments
Abstract
Purpose: To elucidate and compare benefit-risk preferences among Korean patients and physicians concerning cyclooxygenase-2 (Cox-2) inhibitor treatments for arthritis.
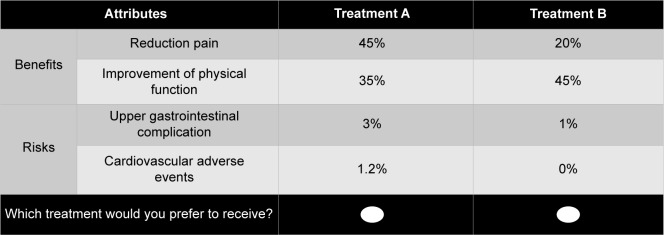
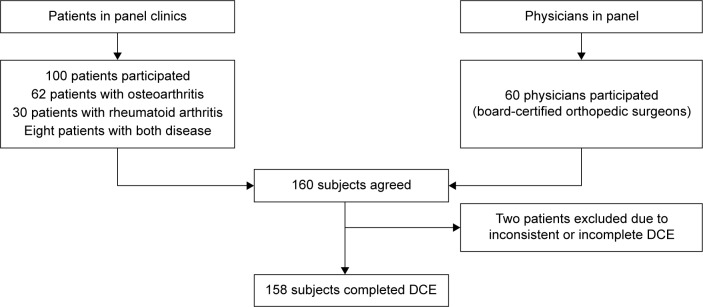
Materials and methods: Subjects included 100 patients with arthritis and 60 board-certified orthopedic surgeon physicians in South Korea. Through a systematic review of the literature, beneficial attributes of using Cox-2 inhibitors were defined as a decrease in the Western Ontario and McMaster Universities Arthritis Index for pain score and improvement in physical function. Likewise, risk attributes included upper gastrointestinal (GI) complications and cardiovascular (CV) adverse events. Discrete choice experiments were used to determine preferences for these four attributes among Korean patients and physicians. Relative importance and maximum acceptable risk for improving beneficial attributes were assessed by analyzing the results of the discrete choice experiment by using a conditional logit model.
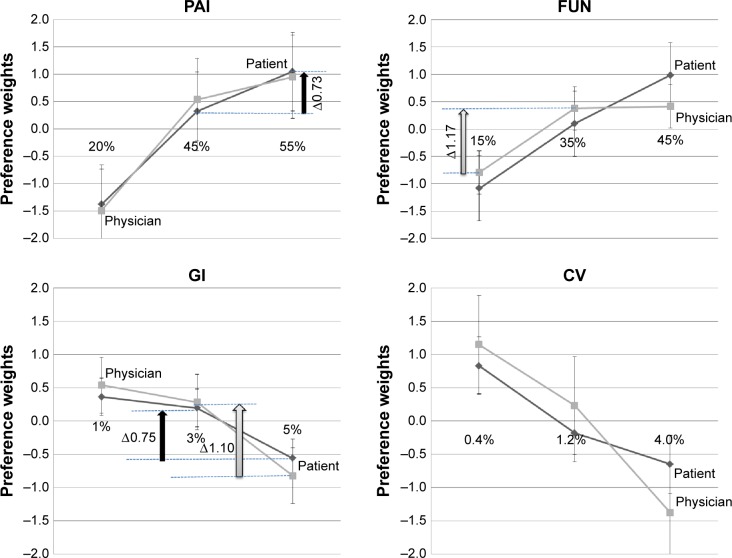
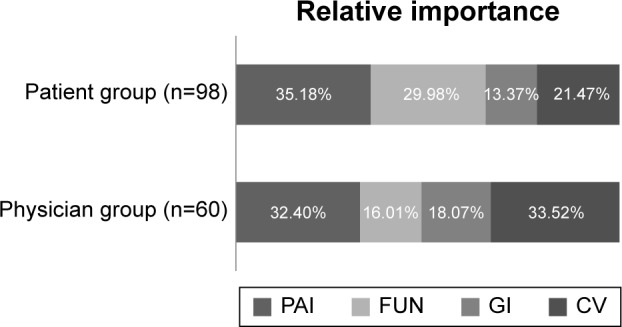
Results: Patients ranked the relative importance of benefit-risk attributes as follows: pain reduction (35.2%); physical function improvement (30.0%); fewer CV adverse events (21.5%); fewer GI complications (13.4%). The physicians' ranking for the same attributes was as follows: fewer CV (33.5%); pain reduction (32.4%); fewer GI complications (18.1%); physical function improvement (16.0%). Patients were more willing than physicians to accept risks when pain improved from 20% or 45% to 55% and physical function improved from 15% or 35% to 45%.
Conclusion: We confirmed that patients and physicians had different benefit-risk preferences regarding Cox-2 inhibitors. Patients with arthritis prioritized the benefits of Cox-2 inhibitors over the risks; moreover, in comparison with the physicians, arthritis patients were more willing to accept the trade-off between benefits and risks to achieve the best treatment level. To reduce the preference gap and achieve treatment goals, physicians must better understand their patients' preferences.
Keywords: Cox-2 inhibitors; arthritis; discrete choice experiment; patient and physicians preference; willingness to accept.
Figures
Similar articles
-
Patient and physician preferences for anticancer drugs for the treatment of metastatic colorectal cancer: a discrete-choice experiment.Cancer Manag Res. 2017 Apr 27;9:149-158. doi: 10.2147/CMAR.S125245. eCollection 2017. Cancer Manag Res. 2017. PMID: 28490902 Free PMC article.
-
Benefit-risk trade-offs for treatment decisions in moderate-to-severe rheumatoid arthritis: focus on the patient perspective.Rheumatol Int. 2017 Sep;37(9):1423-1434. doi: 10.1007/s00296-017-3760-z. Epub 2017 Jun 16. Rheumatol Int. 2017. PMID: 28623526
-
Analysis of physicians' perspectives versus patients' preferences: direct assessment and discrete choice experiments in the therapy of multiple myeloma.Eur J Health Econ. 2011 Jun;12(3):193-203. doi: 10.1007/s10198-010-0218-6. Epub 2010 Jan 28. Eur J Health Econ. 2011. PMID: 20107856
-
The importance of understanding patient and physician preferences for psoriasis treatment characteristics: a systematic review of discrete-choice experiments.Curr Med Res Opin. 2020 Aug;36(8):1257-1275. doi: 10.1080/03007995.2020.1776233. Epub 2020 Jul 1. Curr Med Res Opin. 2020. PMID: 32468865
-
Patient preferences for epilepsy treatment: a systematic review of discrete choice experimental studies.Health Econ Rev. 2023 Mar 18;13(1):17. doi: 10.1186/s13561-023-00431-0. Health Econ Rev. 2023. PMID: 36933108 Free PMC article. Review.
Cited by
-
Patients' Preferences Regarding Osteoarthritis Medications: An Adaptive Choice-Based Conjoint Analysis Study.Patient Prefer Adherence. 2020 Dec 22;14:2501-2515. doi: 10.2147/PPA.S283922. eCollection 2020. Patient Prefer Adherence. 2020. PMID: 33376311 Free PMC article.
-
Incorporating patient preferences into osteoarthritis treatment.Arch Rheumatol. 2021 Oct 16;36(4):577-586. doi: 10.46497/ArchRheumatol.2022.8291. eCollection 2021 Dec. Arch Rheumatol. 2021. PMID: 35382376 Free PMC article.
-
Defined Daily Dose and Appropriateness of Clinical Application: The Coxibs and Traditional Nonsteroidal Anti-Inflammatory Drugs for Postoperative Orthopaedics Pain Control in a Private Hospital in Malaysia.Pharmacy (Basel). 2020 Dec 8;8(4):235. doi: 10.3390/pharmacy8040235. Pharmacy (Basel). 2020. PMID: 33302438 Free PMC article.
-
Preferences for Renal Cell Carcinoma Pharmacological Treatment: A Discrete Choice Experiment in Patients and Oncologists.Front Oncol. 2022 Jan 7;11:773366. doi: 10.3389/fonc.2021.773366. eCollection 2021. Front Oncol. 2022. PMID: 35070976 Free PMC article.
-
Patients' preferences for osteoarthritis treatment: the value of stated-preference studies.Aging Clin Exp Res. 2019 Jan;31(1):1-3. doi: 10.1007/s40520-018-1098-3. Epub 2019 Jan 4. Aging Clin Exp Res. 2019. PMID: 30607878 Free PMC article. No abstract available.
References
-
- Hur NW, Choi CB, Uhm WS, Bae SC. The prevalence and trend of arthritis in Korea: results from Korea National health and nutrition examination surveys. J Korean Rheum Assoc. 2008;15:11–26.
-
- McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage. 2014;22:363–388. - PubMed
-
- Dai C, Stafford RS, Alexander GC. National trends in cyclooxygenase-2 inhibitor use since market release: nonselective diffusion of a selectively cost-effective innovation. Arch Intern Med. 2005;165:171–177. - PubMed
-
- Castellsague J, Riera-Guardia N, Calingaert B, et al. Safety of Non-Steroidal Anti-Inflammatory Drugs (SOS) Project Individual NSAIDs and upper gastrointestinal complications: a systematic review and meta-analysis of observational studies (the SOS project) Drug Saf. 2012;35(12):1127–1146. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
