

Interfascial Dissection for Protection of the Nerve Branches to the Frontalis Muscles during Supraorbital Trans-Eyebrow Approach: An Anatomical Study and Technical Note
- PMID: 27175323
- PMCID: PMC4862837
- DOI: 10.1055/s-0035-1568872
Interfascial Dissection for Protection of the Nerve Branches to the Frontalis Muscles during Supraorbital Trans-Eyebrow Approach: An Anatomical Study and Technical Note
Abstract
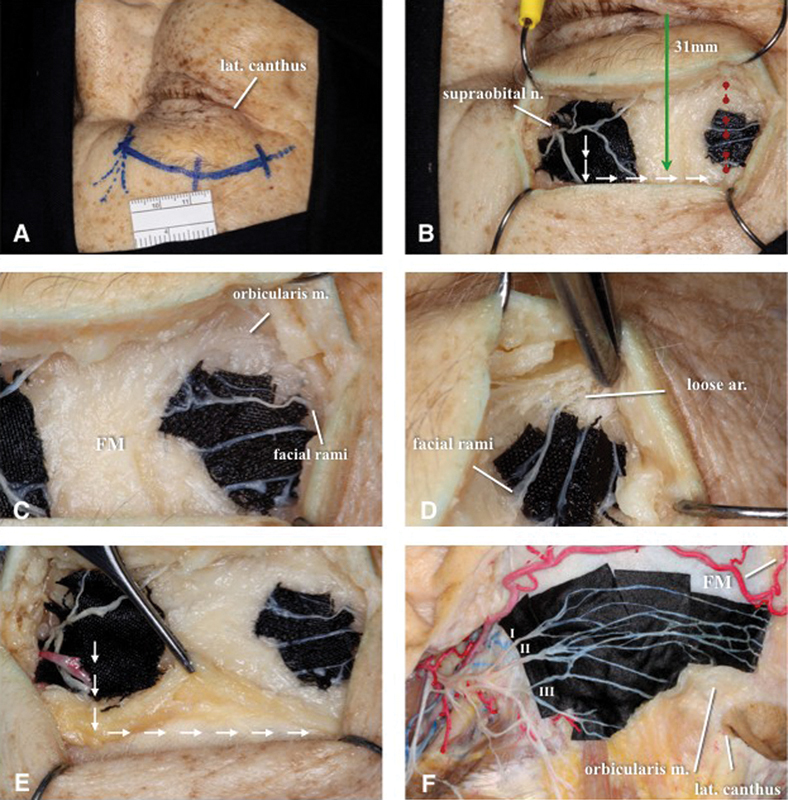
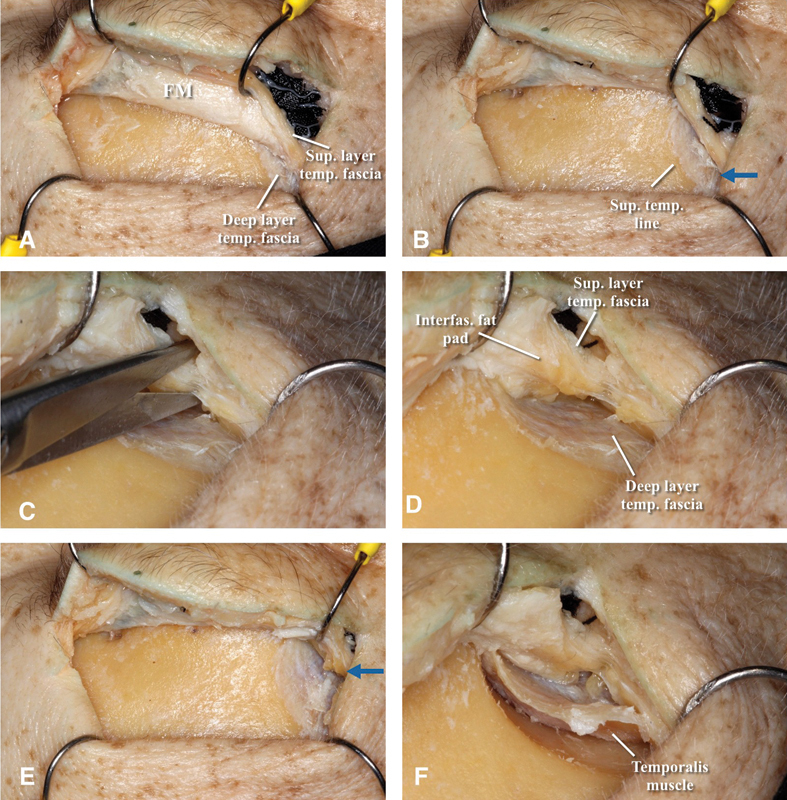
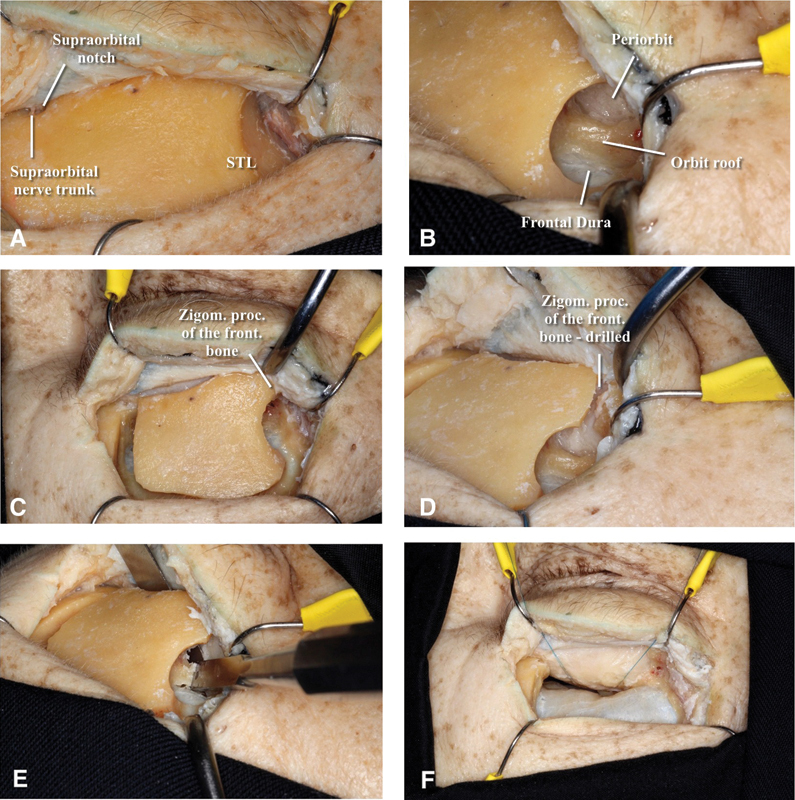
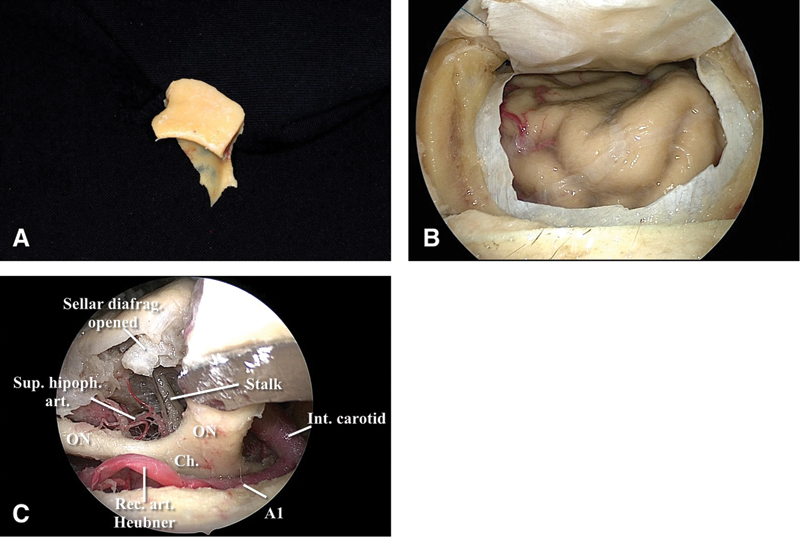
Introduction Preservation of the temporal branches of the facial nerve during anterolateral craniotomies is important. Damaging it can inflict undesirable cosmetic defects to the patient. The supraorbital trans-eyebrow approach (SOTE) is a versatile keyhole craniotomy but still has a high rate of frontalis muscle (FM) palsy. Objective Anatomical study to implement the interfascial dissection during the SOTE to preserve the nerves to the FM. Methods Slight modification of the standard technique of the SOTE was performed in 6 cadaveric specimens (12 sides). Results Distal rami to the FM were exposed. The standard "u-shape" incision of the FM can cross over the nerves. Alternatively, an "l-shape" incision was performed until the superior temporal line (STL). An interfascial dissection was performed near to the STL and the interfascial fat pad was used as a protective layer for the nerves. Conclusion Various pathologies can be addressed with the SOTE. In the majority of the cases the cosmetic results are good, but FM palsy remains a drawback of this approach. The interfascial dissection may be used in an attempt to prevent frontalis rami palsy.
Keywords: frontalis muscle palsy; interfascial dissection; nerve protection; supraorbital trans-eyebrow approach.
Figures
Similar articles
-
Preservation of the nerves to the frontalis muscle during pterional craniotomy.J Neurosurg. 2015 Jun;122(6):1274-82. doi: 10.3171/2014.10.JNS142061. Epub 2015 Apr 3. J Neurosurg. 2015. PMID: 25839922
-
Reappraisal of the anatomy of the frontotemporal branches of the facial nerve.J Neurosurg. 2023 Mar 10;139(4):1160-1168. doi: 10.3171/2023.1.JNS222027. Print 2023 Oct 1. J Neurosurg. 2023. PMID: 36905660
-
Subfascial and submuscular methods of temporal muscle dissection and their relationship to the frontal branch of the facial nerve. Technical note.J Neurosurg. 2000 May;92(5):877-80. doi: 10.3171/jns.2000.92.5.0877. J Neurosurg. 2000. PMID: 10794306
-
A Review of the Literature on the Transciliary Supraorbital Keyhole Approach.World Neurosurg. 2017 Feb;98:614-624. doi: 10.1016/j.wneu.2016.10.110. Epub 2016 Oct 27. World Neurosurg. 2017. PMID: 27989977 Review.
-
Median Supraorbital Keyhole Approach for Clipping Ruptured Distal Anterior Cerebral Artery Aneurysm: Technical Report with Review of Literature.World Neurosurg. 2018 Apr;112:73-76. doi: 10.1016/j.wneu.2018.01.100. Epub 2018 Feb 2. World Neurosurg. 2018. PMID: 29410300 Review.
Cited by
-
Orbital Anatomy: Anatomical Relationships of Surrounding Structures.J Neurol Surg B Skull Base. 2020 Aug;81(4):333-347. doi: 10.1055/s-0040-1713931. Epub 2020 Aug 24. J Neurol Surg B Skull Base. 2020. PMID: 33072475 Free PMC article.
-
Treatment of post-craniotomy acute severe supraorbital neuralgia using ultrasound-guided pulsed radiofrequency: a case report.J Pain Res. 2018 Aug 8;11:1497-1501. doi: 10.2147/JPR.S166446. eCollection 2018. J Pain Res. 2018. PMID: 30122980 Free PMC article.
-
The extradural minipterional approach for the treatment of paraclinoid aneurysms: a cadaver stepwise dissection and clinical case series.Neurosurg Rev. 2020 Feb;43(1):361-370. doi: 10.1007/s10143-019-01219-9. Epub 2019 Dec 9. Neurosurg Rev. 2020. PMID: 31820141
-
Same viewing angle, minimal craniotomy enlargement, extreme exposure increase: the extended supraorbital eyebrow approach.Neurosurg Rev. 2021 Apr;44(2):1141-1150. doi: 10.1007/s10143-020-01306-2. Epub 2020 May 11. Neurosurg Rev. 2021. PMID: 32394302
References
-
- Babakurban S T, Cakmak O, Kendir S, Elhan A, Quatela V C. Temporal branch of the facial nerve and its relationship to fascial layers. Arch Facial Plast Surg. 2010;12(1):16–23. - PubMed
-
- Ammirati M Spallone A Ma J Cheatham M Becker D An anatomicosurgical study of the temporal branch of the facial nerve Neurosurgery 19933361038–1043., discussion 1044 - PubMed
-
- Coscarella E, Vishteh A G, Spetzler R F, Seoane E, Zabramski J M. Subfascial and submuscular methods of temporal muscle dissection and their relationship to the frontal branch of the facial nerve. Technical note. J Neurosurg. 2000;92(5):877–880. - PubMed
-
- Yaşargil M G, Reichman M V, Kubik S. Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. Technical article. J Neurosurg. 1987;67(3):463–466. - PubMed
-
- Ammirati M, Spallone A, Ma J, Cheatham M, Becker D. Preservation of the temporal branch of the facial nerve in pterional-transzygomatic craniotomy. Acta Neurochir (Wien) 1994;128(1–4):163–165. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
