

A Challenging Surgical Approach to Locally Advanced Primary Urethral Carcinoma: A Case Report and Literature Review
- PMID: 27175683
- PMCID: PMC4902525
- DOI: 10.1097/MD.0000000000003642
A Challenging Surgical Approach to Locally Advanced Primary Urethral Carcinoma: A Case Report and Literature Review
Abstract
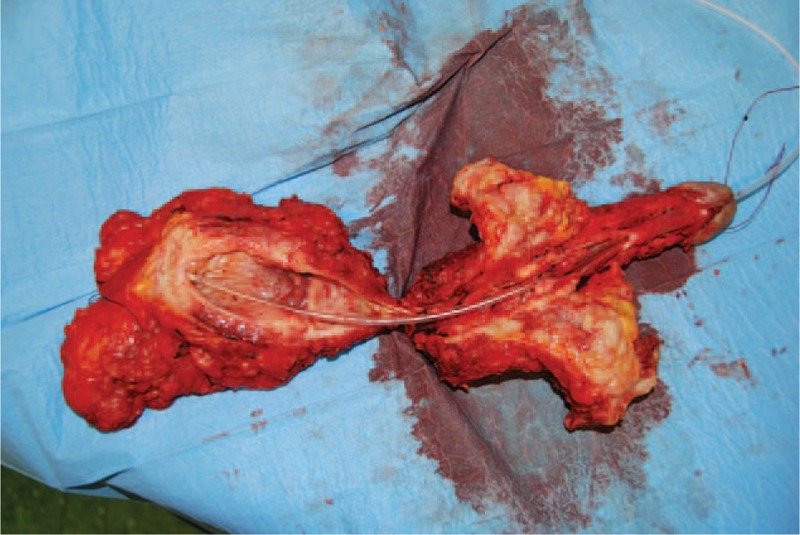
Primary urethral carcinoma (PUC) is a rare and aggressive cancer, often underdetected and consequently unsatisfactorily treated. We report a case of advanced PUC, surgically treated with combined approaches.A 47-year-old man underwent transurethral resection of a urethral lesion with histological evidence of a poorly differentiated squamous cancer of the bulbomembranous urethra. Computed tomography (CT) and bone scans excluded metastatic spread of the disease but showed involvement of both corpora cavernosa (cT3N0M0). A radical surgical approach was advised, but the patient refused this and opted for chemotherapy. After 17 months the patient was referred to our department due to the evidence of a fistula in the scrotal area. CT scan showed bilateral metastatic disease in the inguinal, external iliac, and obturator lymph nodes as well as the involvement of both corpora cavernosa. Additionally, a fistula originating from the right corpus cavernosum extended to the scrotal skin. At this stage, the patient accepted the surgical treatment, consisting of different phases. Phase I: Radical extraperitoneal cystoprostatectomy with iliac-obturator lymph nodes dissection. Phase II: Creation of a urinary diversion through a Bricker ileal conduit. Phase III: Repositioning of the patient in lithotomic position for an overturned Y skin incision, total penectomy, fistula excision, and "en bloc" removal of surgical specimens including the bladder, through the perineal breach. Phase IV: Right inguinal lymphadenectomy.The procedure lasted 9-and-a-half hours, was complication-free, and intraoperative blood loss was 600 mL. The patient was discharged 8 days after surgery. Pathological examination documented a T4N2M0 tumor. The clinical situation was stable during the first 3 months postoperatively but then metastatic spread occurred, not responsive to adjuvant chemotherapy, which led to the patient's death 6 months after surgery.Patients with advanced stage tumors of the bulbomembranous urethra should be managed with radical surgery including the corporas up to the ischiatic tuberosity attachment, and membranous urethra in continuity with the prostate and bladder. Neo-adjuvant treatment may be advisable with the aim of improving the poor prognosis, even if the efficacy is not certain while it can delay the radical treatment of the disease.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures




References
-
- Swartz MA, Porter MP, Lin DW, et al. Incidence of primary urethral carcinoma in the United States. Urology 2006; 68:1164–1168. - PubMed
-
- Visser O, Adolfsson J, Rossi S, et al. Incidence and survival of rare urogenital cancers in Europe. Eur J Cancer 2012; 48:456–464. - PubMed
-
- Rabbani F. Prognostic factors in male urethral cancer. Cancer 2011; 117:2426–2434. - PubMed
-
- National Cancer Institute, Division of Cancer Control and Population Sciences, Surveillance Research Program, Cancer Statistics Branch. Surveillance, Epidemiology, and End Results (SEER) Program. www.seer.cancer.gov Accessed February 01, 2016.
-
- Dalbagni G, Zhang Z, Lacombe L, et al. Male urethral carcinoma: analysis of treatment outcome. J Urol 1999; 53:1126–1132. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
