

The cost-effectiveness of tumor-treating fields therapy in patients with newly diagnosed glioblastoma
- PMID: 27177573
- PMCID: PMC4933490
- DOI: 10.1093/neuonc/now102
The cost-effectiveness of tumor-treating fields therapy in patients with newly diagnosed glioblastoma
Abstract
Background: There is strong concern about the costs associated with adding tumor-treating fields (TTF) therapy to standard first-line treatment for glioblastoma (GBM). Hence, we aimed to determine the cost-effectiveness of TTF therapy for the treatment of newly diagnosed patients with GBM.
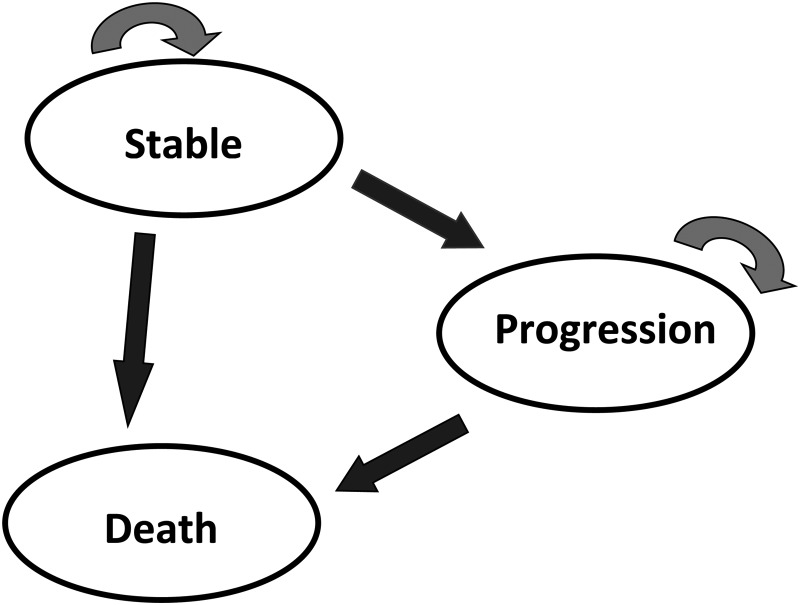
Methods: We developed a 3-health-state Markov model. The perspective was that of the French Health Insurance, and the horizon was lifetime. We calculated the transition probabilities from the survival parameters reported in the EF-14 trial. The main outcome measure was incremental effectiveness expressed as life-years gained (LYG). Input costs were derived from the literature. We calculated the incremental cost-effectiveness ratio (ICER) expressed as cost/LYG. We used 1-way deterministic and probabilistic sensitivity analysis to evaluate the model uncertainty.
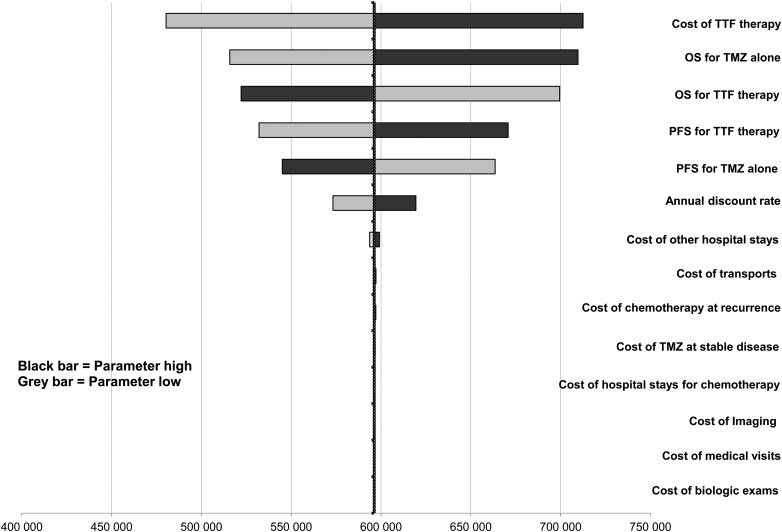
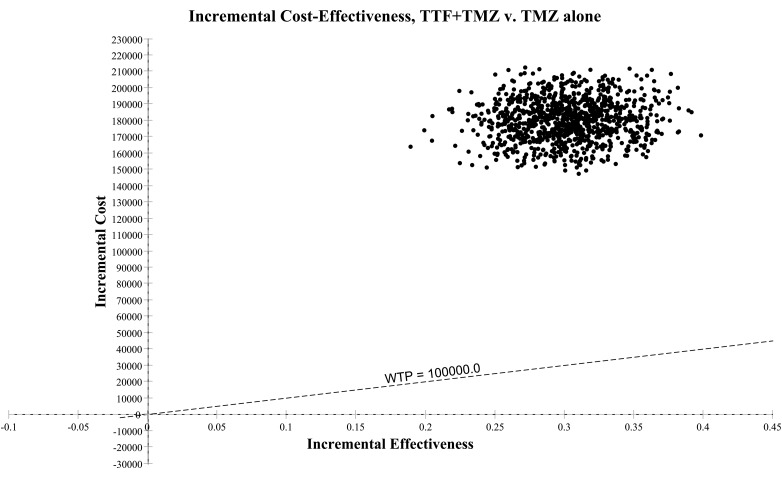
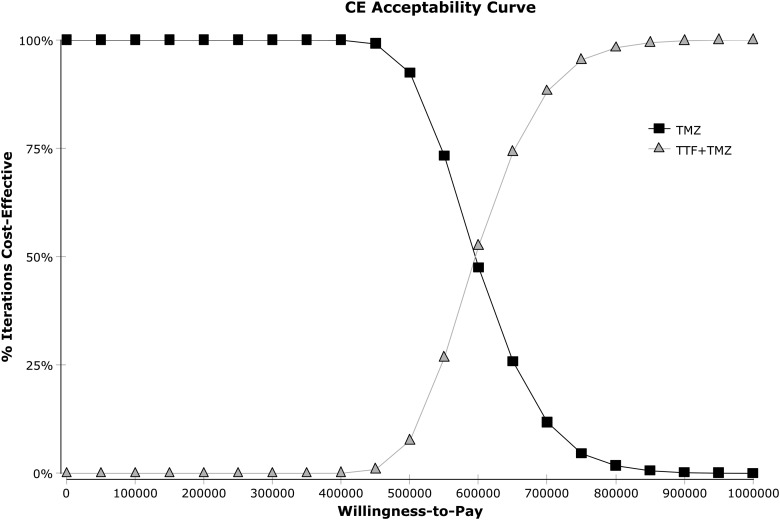
Results: In the base-case analysis, adding TTF therapy to standard of care resulted in increases of life expectancy of 4.08 months (0.34 LYG) and €185 476 per patient. The ICER was €549 909/LYG. The discounted ICER was €596 411/LYG. Parameters with the most influence on ICER were the cost of TTF therapy, followed equally by overall survival and progression-free survival in both arms. The probabilistic sensitivity analysis showed a 95% confidence interval of the ICER of €447 017/LYG to €745 805/LYG with 0% chance to be cost-effective at a threshold of €100 000/LYG.
Conclusion: The ICER of TTF therapy at first-line treatment is far beyond conventional thresholds due to the prohibitive announced cost of the device. Strong price regulation by health authorities could make this technology more affordable and consequently accessible to patients.
Keywords: brain tumor; cost-effectiveness analysis; glioblastoma; temozolomide; tumor-treating fields.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Living in a material world: tumor-treating fields at the top of the charts.Neuro Oncol. 2016 Aug;18(8):1033-4. doi: 10.1093/neuonc/now138. Neuro Oncol. 2016. PMID: 27382117 Free PMC article. No abstract available.
References
-
- Stupp R, Brada M, van den Bent MJ, Tonn JC, Pentheroudakis ESMO Guidelines Working Group. . High-grade glioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25 Suppl 3:iii93–ii101. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Chinot OL, Wick W, Mason W et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N Engl J Med. 2014;370(8):709–722. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
