

Pooled analyses of eribulin in metastatic breast cancer patients with at least one prior chemotherapy
- PMID: 27177860
- PMCID: PMC4959925
- DOI: 10.1093/annonc/mdw203
Pooled analyses of eribulin in metastatic breast cancer patients with at least one prior chemotherapy
Abstract
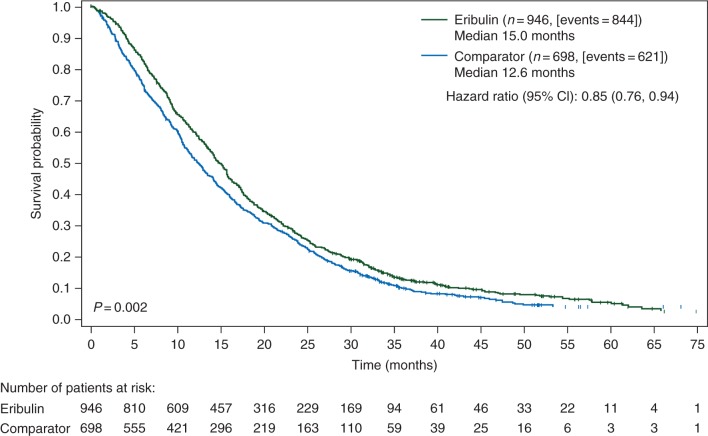
Background: Based on data from two multicenter, phase III clinical trials (Studies 301 and 305), eribulin (a microtubule dynamics inhibitor) is indicated in the European Union (EU) for patients with locally advanced or metastatic breast cancer (MBC) after ≥1 prior chemotherapy for advanced disease, including an anthracycline and a taxane in either the adjuvant or metastatic setting. Data from Studies 305 and 301 were pooled to investigate the efficacy of eribulin in various subgroups of patients who matched the EU label, including those with human epidermal growth factor receptor 2 (HER2)-negative and triple-negative disease.
Patients and methods: In Study 305 (NCT00388726), patients were randomized 2:1 to eribulin mesylate 1.4 mg/m(2) (equivalent to eribulin 1.23 mg/m(2) [expressed as free base]) intravenously on days 1 and 8 every 21 days] or treatment of physician's choice after 2-5 prior chemotherapies (≥2 for advanced disease), including an anthracycline and a taxane (in early/advanced setting). In Study 301 (NCT00337103), patients were randomized 1:1 to eribulin (as above) or capecitabine (1.25 g/m(2) orally twice daily on days 1-14 every 21 days) following ≤3 prior chemotherapies (≤2 for advanced disease), including an anthracycline and a taxane. Efficacy end points were investigated in the intent-to-treat population and subgroups, pooled as discussed above.
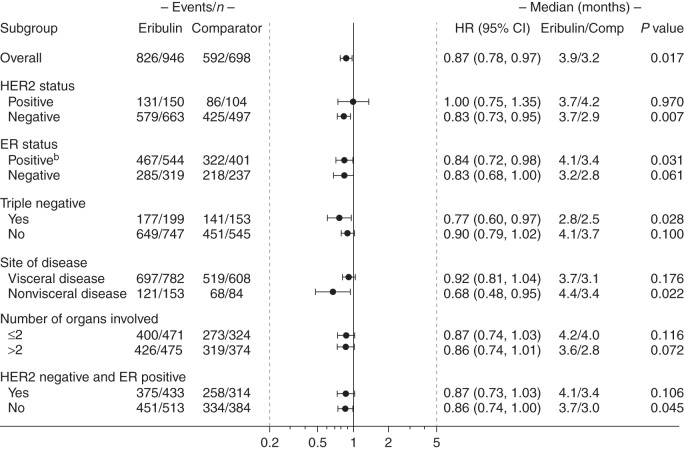
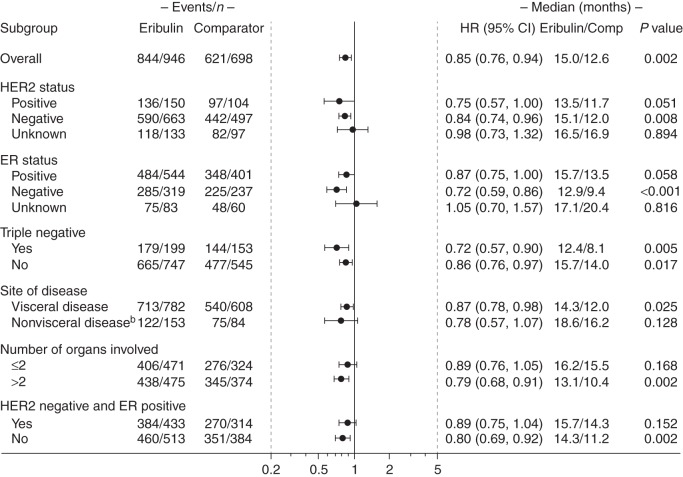
Results: Overall, 1644 patients were included (eribulin: 946; control: 698); baseline characteristics were well matched. Overall survival was significantly longer with eribulin versus control (P < 0.01), as were progression-free survival and clinical benefit rate (both P < 0.05). Significant survival benefits with eribulin versus control were observed in a wide range of patient subgroups, including HER2-negative or triple-negative disease (all P < 0.05).
Conclusion: Our findings underline the survival benefit achieved by eribulin used according to EU label in the overall MBC population and in various subgroups of interest, including patients with HER2-negative and triple-negative disease.
Keywords: clinical trial; eribulin; metastatic breast cancer; pooled analysis; survival; triple-negative breast cancer.
© The Author 2016. Published by Oxford University Press on behalf of the European Society for Medical Oncology. .
Figures
References
-
- SEER Cancer Statistics Factsheets: Female Breast Cancer. Bethesda, MD: National Cancer Institute; http://seer.cancer.gov/statfacts/html/breast.html (5 November 2015, date last accessed).
-
- National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Breast Cancer; Version 3.2015. http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (5 November 2015, date last accessed).
-
- Cortes J, O'Shaughnessy J, Loesch D et al. . Eribulin monotherapy versus treatment of physician's choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Lancet 2011; 377: 914–923. - PubMed
-
- Halaven 0.44 mg/ml solution for injection [summary of product characteristics]. Hertfordshire, UK: Eisai Europe Limited.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
