

Intestinal perforation management using T-tube drainage
- PMID: 27177890
- PMCID: PMC4866283
- DOI: 10.1093/jscr/rjw085
Intestinal perforation management using T-tube drainage
Abstract
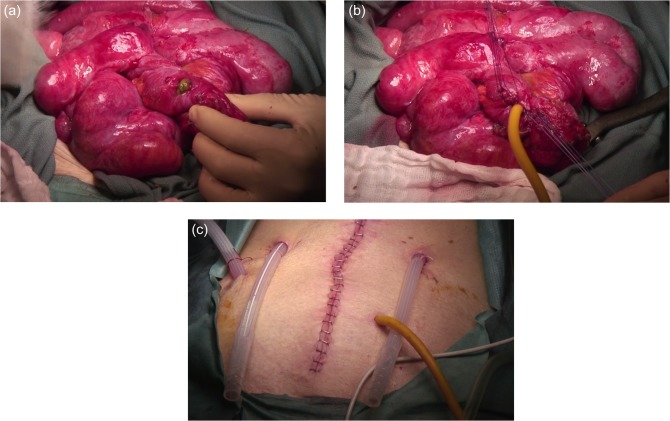
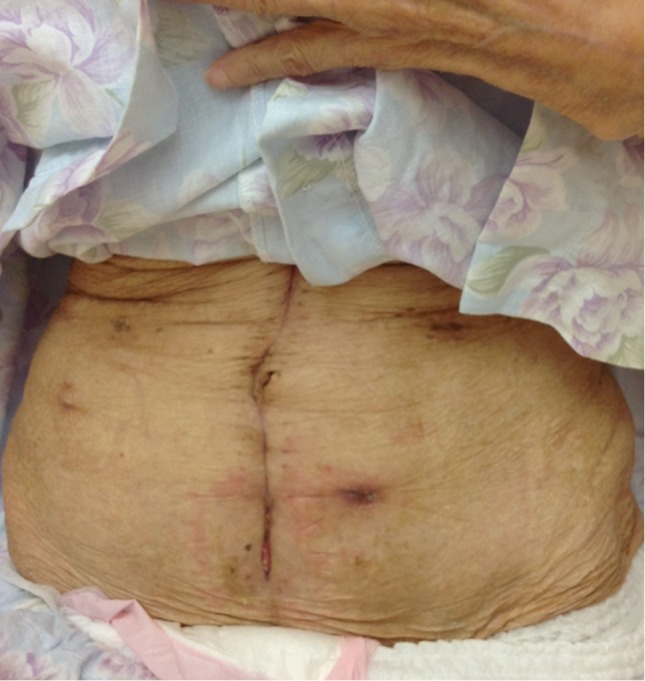
In cases of small bowel perforation with gross contamination, enterostomy has traditionally been the treatment of choice. An 86-year-old woman was diagnosed with perforative peritonitis. Emergency laparotomy revealed a small bowel perforation with gross contamination, and a T-tube enterostomy was performed. The T-tube was used for intestinal decompression for the first few days and was then accompanied by enteral feeding. When oral intake was sufficient, the T-tube was removed. The abdominal wall's fistula healed within 2 days of removal. Except for wound infection, the patient developed no postoperative complications. Under specific circumstances, a T-tube enterostomy can be an effective alternative for a traditional enterostomy. Its advantages include less or no anastomotic leakage, easier management of fluid and electrolyte levels, postoperative enteral feeding from the tube, a shorter operative time and no need for a second operation to close the stoma.
Published by Oxford University Press and JSCR Publishing Ltd. All rights reserved. © The Author 2016.
Figures
Similar articles
-
[Analysis on operational safety of chronic radiation intestinal injury].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Nov 25;22(11):1034-1040. doi: 10.3760/cma.j.issn.1671-0274.2019.11.006. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31770834 Chinese.
-
A pilot study on prophylactic tube enterostomy for the prevention of anastomotic leakage in patients with high-risk intestinal anastomosis.Langenbecks Arch Surg. 2022 Feb;407(1):267-275. doi: 10.1007/s00423-021-02326-2. Epub 2021 Sep 21. Langenbecks Arch Surg. 2022. PMID: 34549336
-
Foley catheter enterostomy for postoperative bowel perforation: an effective source control.World J Surg. 2010 Nov;34(11):2752-4. doi: 10.1007/s00268-010-0741-8. World J Surg. 2010. PMID: 20703469
-
Palliative Chemotherapy: Does It Only Provide False Hope? The Role of Palliative Care in a Young Patient With Newly Diagnosed Metastatic Adenocarcinoma.J Adv Pract Oncol. 2017 May-Jun;8(4):382-386. Epub 2017 May 1. J Adv Pract Oncol. 2017. PMID: 30018843 Free PMC article. Review.
-
The surgical management of necrotising enterocolitis.Early Hum Dev. 2005 Jan;81(1):79-85. doi: 10.1016/j.earlhumdev.2004.10.018. Early Hum Dev. 2005. PMID: 15707718 Review.
References
-
- Pandey A, Kumar V, Gangopadhyay AN, Upadhyaya VD, Srivastava A, Singh RB. A pilot study on the role of T-tube in typhoid ileal perforation in children. World J Surg 2008;32:2607–11. - PubMed
-
- Ceelen W, Hesse U, Hemptinne BD. Small bowel perforation following blunt abdominal trauma. Acta Chir Belg 1995;95:187–9. - PubMed
-
- Seyfarth T, Baumgartner I, Triller J, Dinkel HP. Accidental small bowel perforation after antegrade femoral artery access for percutaneous thromboembolectomy and angioplasty. J Endovasc Ther 2002;9:685–9. - PubMed
-
- Rygl M, Pycha K, Stranak Z, Skaba R, Brabec R, Cunat V, et al. . T-tube ileostomy for intestinal perforation in extremely low birth weight neonates. Pediatr Surg Int 2007;23:685–8. - PubMed
-
- Miller BJ, Schache DJ. Colorectal injury: where do we stand with repair. Aust NZ J Surg 1996;66:348–52. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
