

Cost-Effectiveness of Field Trauma Triage among Injured Adults Served by Emergency Medical Services
- PMID: 27178369
- PMCID: PMC4975576
- DOI: 10.1016/j.jamcollsurg.2016.02.014
Cost-Effectiveness of Field Trauma Triage among Injured Adults Served by Emergency Medical Services
Abstract
Background: The American College of Surgeons Committee on Trauma sets national targets for the accuracy of field trauma triage at ≥95% sensitivity and ≥65% specificity, yet the cost-effectiveness of realizing these goals is unknown. We evaluated the cost-effectiveness of current field trauma triage practices compared with triage strategies consistent with the national targets.
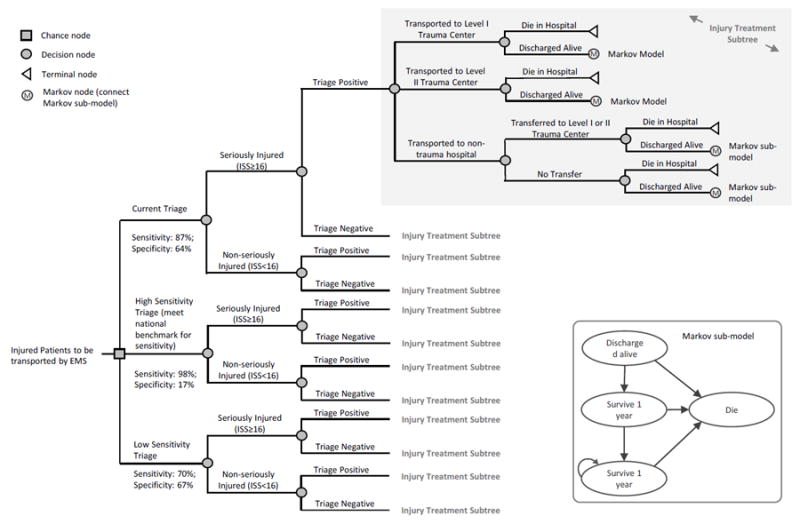
Study design: This was a cost-effectiveness analysis using data from 79,937 injured adults transported by 48 emergency medical services agencies to 105 trauma and nontrauma hospitals in 6 regions of the western United States from 2006 through 2008. Incremental differences in survival, quality-adjusted life years (QALYs), costs, and the incremental cost-effectiveness ratio (costs per QALY gained) were estimated for each triage strategy during a 1-year and lifetime horizon using a decision analytic Markov model. We considered an incremental cost-effectiveness ratio threshold of <$100,000 to be cost-effective.
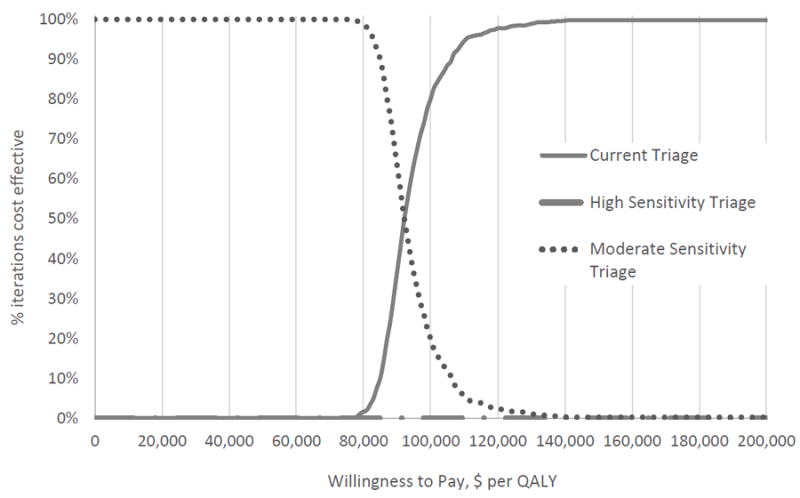
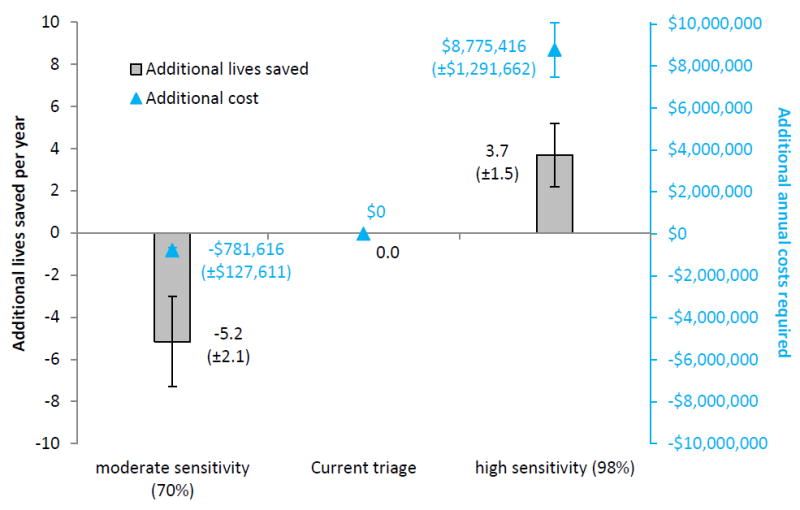
Results: For these 6 regions, a high-sensitivity triage strategy consistent with national trauma policy (sensitivity 98.6%, specificity 17.1%) would cost $1,317,333 per QALY gained, and current triage practices (sensitivity 87.2%, specificity 64.0%) cost $88,000 per QALY gained, compared with a moderate sensitivity strategy (sensitivity 71.2%, specificity 66.5%). Refining emergency medical services transport patterns by triage status improved cost-effectiveness. At the trauma-system level, a high-sensitivity triage strategy would save 3.7 additional lives per year at a 1-year cost of $8.78 million, and a moderate sensitivity approach would cost 5.2 additional lives and save $781,616 each year.
Conclusions: A high-sensitivity approach to field triage consistent with national trauma policy is not cost-effective. The most cost-effective approach to field triage appears closely tied to triage specificity and adherence to triage-based emergency medical services transport practices.
Copyright © 2016 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wang HE, Mann NC, Jacobson KE, et al. National characteristics of emergency medical services responses in the United States. Prehosp Emerg Care. 2013;17:8–14. - PubMed
-
- Sasser SM, Hunt RC, Faul M, et al. MMWR Recommendations and reports : Morbidity and mortality weekly report. RR-1. Vol. 61. Recommendations and reports / Centers for Disease Control; Jan 13, 2012. Guidelines for field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2011; pp. 1–20. - PubMed
-
- Mackersie RC. History of trauma field triage development and the American College of Surgeons criteria. Prehosp Emerg Care. 2006;10:287–294. - PubMed
-
- Haas B, Gomez D, Zagorski B, et al. Survival of the fittest: the hidden cost of undertriage of major trauma. J Am Coll Surg. 2010;211:804–811. - PubMed
-
- Haas B, Stukel TA, Gomez D, et al. The mortality benefit of direct trauma center transport in a regional trauma system: a population-based analysis. J Trauma Acute Care Surg. 2012;72:1510–1515. discussion 1515-1517. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
