

Effects of a risk-based online mammography intervention on accuracy of perceived risk and mammography intentions
- PMID: 27178707
- PMCID: PMC5028247
- DOI: 10.1016/j.pec.2016.05.005
Effects of a risk-based online mammography intervention on accuracy of perceived risk and mammography intentions
Abstract
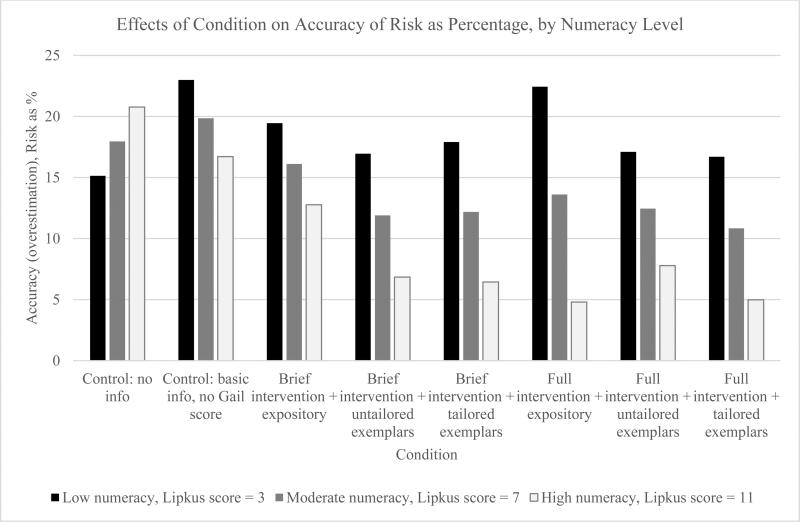
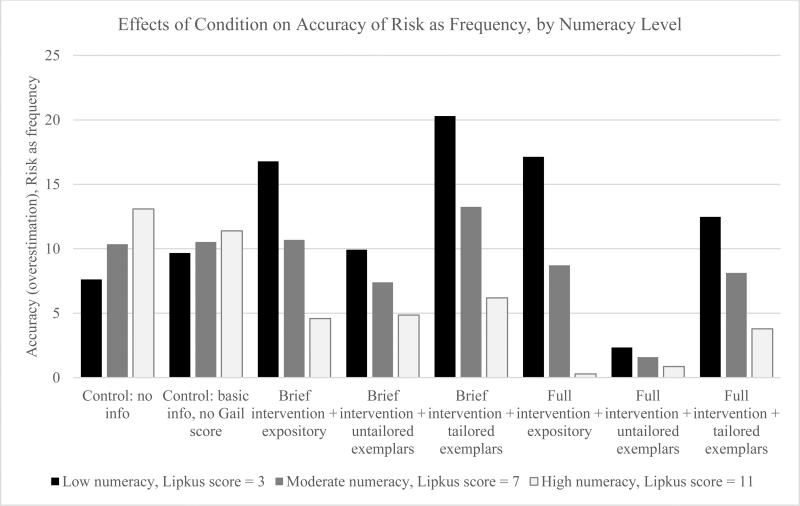
Objective: This experiment tested the effects of an individualized risk-based online mammography decision intervention. The intervention employs exemplification theory and the Elaboration Likelihood Model of persuasion to improve the match between breast cancer risk and mammography intentions.
Methods: 2918 women ages 35-49 were stratified into two levels of 10-year breast cancer risk (<1.5%; ≥1.5%) then randomly assigned to one of eight conditions: two comparison conditions and six risk-based intervention conditions that varied according to a 2 (amount of content: brief vs. extended) x 3 (format: expository vs. untailored exemplar [example case] vs. tailored exemplar) design. Outcomes included mammography intentions and accuracy of perceived breast cancer risk.
Results: Risk-based intervention conditions improved the match between objective risk estimates and perceived risk, especially for high-numeracy women with a 10-year breast cancer risk ≤1.5%. For women with a risk≤1.5%, exemplars improved accuracy of perceived risk and all risk-based interventions increased intentions to wait until age 50 to screen.
Conclusion: A risk-based mammography intervention improved accuracy of perceived risk and the match between objective risk estimates and mammography intentions.
Practice implications: Interventions could be applied in online or clinical settings to help women understand risk and make mammography decisions.
Keywords: Communication intervention; Decision aid; Mammography; Numeracy; Perceived risk; Risk communication.
Copyright © 2016 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- U.S. Preventive Services Task Force Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151:716. - PubMed
-
- American College of Obstetricians-Gynecologists Practice bulletin no. 122: breast cancer screening. Obstet Gynecol. 2011 Aug;118:372–82. - PubMed
-
- Mainiero MB, Lourenco A, Mahoney MC, Newell MS, Bailey L, Barke LD, et al. ACR Appropriateness Criteria Breast Cancer Screening. J Am Coll Radiol. 2013 Jan;10:11–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
