

A randomized controlled, non-inferiority trial of modified natural versus artificial cycle for cryo-thawed embryo transfer
- PMID: 27179265
- PMCID: PMC5853593
- DOI: 10.1093/humrep/dew120
A randomized controlled, non-inferiority trial of modified natural versus artificial cycle for cryo-thawed embryo transfer
Abstract
Study question: Are live birth rates (LBRs) after artificial cycle frozen-thawed embryo transfer (AC-FET) non-inferior to LBRs after modified natural cycle frozen-thawed embryo transfer (mNC-FET)?
Summary answer: AC-FET is non-inferior to mNC-FET with regard to LBRs, clinical and ongoing pregnancy rates (OPRs) but AC-FET does result in higher cancellation rates.
What is already known: Pooling prior retrospective studies of AC-FET and mNC-FET results in comparable pregnancy and LBRs. However, these results have not yet been confirmed by a prospective randomized trial.
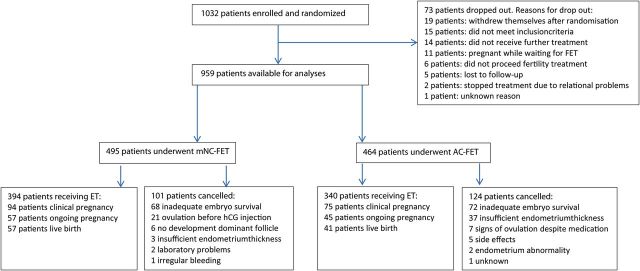
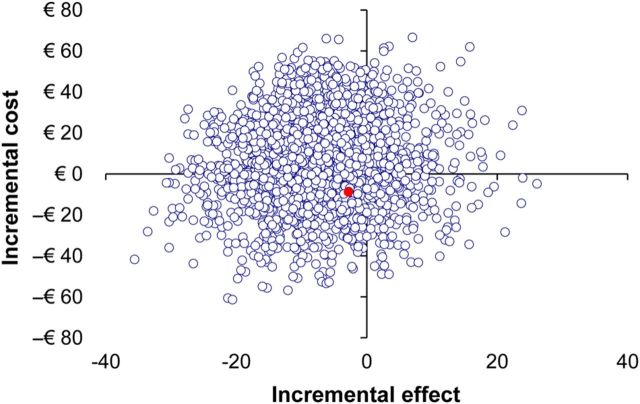
Study design, size and duration: In this non-inferiority prospective randomized controlled trial (acronym 'ANTARCTICA' trial), conducted from February 2009 to April 2014, 1032 patients were included of which 959 were available for analysis. The primary outcome of the study was live birth. Secondary outcomes were clinical and ongoing pregnancy, cycle cancellation and endometrium thickness. A cost-efficiency analysis was performed.
Participant/materials, setting, methods: This study was conducted in both secondary and tertiary fertility centres in the Netherlands. Patients included in this study had to be 18-40 years old, had to have a regular menstruation cycle between 26 and 35 days and frozen-thawed embryos to be transferred had to derive from one of the first three IVF or IVF-ICSI treatment cycles. Patients with a uterine anomaly, a contraindication for one of the prescribed medications in this study or patients undergoing a donor gamete procedure were excluded from participation. Patients were randomized based on a 1:1 allocation to either one cycle of mNC-FET or AC-FET. All embryos were cryopreserved using a slow-freeze technique.
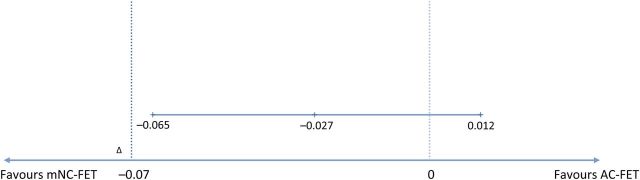
Main results and the role of chance: LBR after mNC-FET was 11.5% (57/495) versus 8.8% in AC-FET (41/464) resulting in an absolute difference in LBR of -0.027 in favour of mNC-FET (95% confidence interval (CI) -0.065-0.012; P = 0.171). Clinical pregnancy occurred in 94/495 (19.0%) patients in mNC-FET versus 75/464 (16.0%) patients in AC-FET (odds ratio (OR) 0.8, 95% CI 0.6-1.1, P = 0.25). 57/495 (11.5%) mNC-FET resulted in ongoing pregnancy versus 45/464 (9.6%) AC-FET (OR 0.7, 95% CI 0.5-1.1, P = 0.15). χ(2) test confirmed the lack of superiority. Significantly more cycles were cancelled in AC-FET (124/464 versus 101/495, OR 1.4, 95% CI 1.1-1.9, P = 0.02). The costs of each of the endometrial preparation methods were comparable (€617.50 per cycle in NC-FET versus €625.73 per cycle in AC-FET, P = 0.54).
Limitations, reasons for caution: The minimum of 1150 patients required for adequate statistical power was not achieved. Moreover, LBRs were lower than anticipated in the sample size calculation.
Wider implications of the findings: LBRs after AC-FET were not inferior to those achieved by mNC-FET. No significant differences in clinical and OPR were observed. The costs of both treatment approaches were comparable.
Study funding/competing interests: An educational grant was received during the conduct of this study. Merck Sharpe Dohme had no influence on the design, execution and analyses of this study. E.R.G. received an education grant by Merck Sharpe Dohme (MSD) during the conduct of the present study. B.J.C. reports grants from MSD during the conduct of the study. A.H. reports grants from MSD and Ferring BV the Netherlands and personal fees from MSD. Grants from ZonMW, the Dutch Organization for Health Research and Development. J.S.E.L. reports grants from Ferring, MSD, Organon, Merck Serono and Schering-Plough during the conduct of the study. F.J.M.B. receives monetary compensation as member of the external advisory board for Merck Serono, consultancy work for Gedeon Richter, educational activities for Ferring BV, research cooperation with Ansh Labs and a strategic cooperation with Roche on automated anti Mullerian hormone assay development. N.S.M. reports receiving monetary compensations for external advisory and speaking work for Ferring BV, MSD, Anecova and Merck Serono during the conduct of the study. All reported competing interests are outside the submitted work. No other relationships or activities that could appear to have influenced the submitted work.
Trial registration number: Netherlands trial register, number NTR 1586.
Trial registration date: 13 January 2009.
First patient included: 20 April 2009.
Keywords: artificial cycle; assisted reproductive techniques; frozen-thawed embryo transfer; in vitro fertilization; modified natural cycle.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
The impact of an inappropriate non-inferiority margin in a non-inferiority trial.Hum Reprod. 2016 Dec;31(12):2892-2893. doi: 10.1093/humrep/dew256. Epub 2016 Oct 14. Hum Reprod. 2016. PMID: 27742724 No abstract available.
-
Reply: The impact of an inappropriate non-inferiority margin in a non-inferiority trial.Hum Reprod. 2016 Dec;31(12):2893. doi: 10.1093/humrep/dew258. Epub 2016 Oct 14. Hum Reprod. 2016. PMID: 27742725 No abstract available.
-
Perspectives on results from cryopreservation/thawing cycles.Hum Reprod. 2016 Dec;31(12):2894. doi: 10.1093/humrep/dew255. Epub 2016 Oct 15. Hum Reprod. 2016. PMID: 27744379 No abstract available.
-
Reply: Perspectives on results from cryopreservation/thawing cycles.Hum Reprod. 2016 Dec;31(12):2894-2895. doi: 10.1093/humrep/dew257. Epub 2016 Oct 15. Hum Reprod. 2016. PMID: 27744380 No abstract available.
References
-
- Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: proceedings of an expert meeting .Hum Reprod 2011;26:1270–1283. - PubMed
-
- Bjuresten K, Landgren BM, Hovatta O, Stavreus-Evers A. Luteal phase progesterone increases live birth rate after frozen embryo transfer .Fertil Steril 2011;95:534–537. - PubMed
-
- Committee for Medicinal Products for Human Use, Efficacy Working Party and Committee for Release for Consultation. Committee for Medicinal Products for Human Use (CHMP) guideline on the choice of the non-inferiority margin .Stat Med 2006;25:1628–1638. - PubMed
-
- Debrock S, Peeraer K, Fernandez Gallardo E, De Neubourg D, Spiessens C, D'Hooghe TM. Vitrification of cleavage stage Day 3 embryos results in higher live birth rates than conventional slow freezing: a RCT. Hum Reprod 2015;30:1820–1830. - PubMed
-
- Edgar DH, Gook DA. A critical appraisal of cryopreservation (slow cooling versus vitrification) of human oocytes and embryos .Hum Reprod Update 2012;18:536–554. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
