

Effect of Noninvasive Ventilation Delivered by Helmet vs Face Mask on the Rate of Endotracheal Intubation in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial
- PMID: 27179847
- PMCID: PMC4967560
- DOI: 10.1001/jama.2016.6338
Effect of Noninvasive Ventilation Delivered by Helmet vs Face Mask on the Rate of Endotracheal Intubation in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial
Abstract
Importance: Noninvasive ventilation (NIV) with a face mask is relatively ineffective at preventing endotracheal intubation in patients with acute respiratory distress syndrome (ARDS). Delivery of NIV with a helmet may be a superior strategy for these patients.
Objective: To determine whether NIV delivered by helmet improves intubation rate among patients with ARDS.
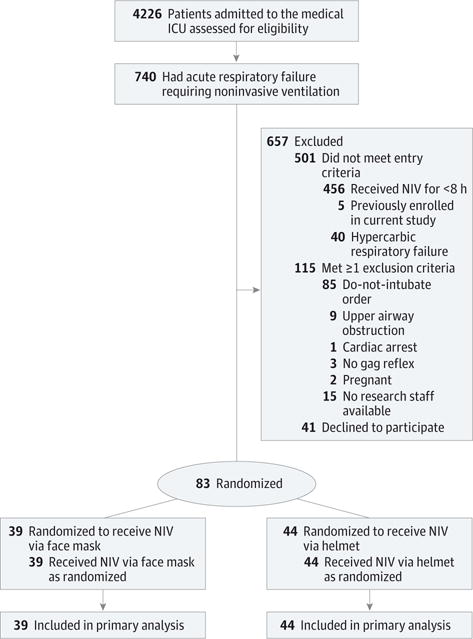
Design, setting, and participants: Single-center randomized clinical trial of 83 patients with ARDS requiring NIV delivered by face mask for at least 8 hours while in the medical intensive care unit at the University of Chicago between October 3, 2012, through September 21, 2015.
Interventions: Patients were randomly assigned to continue face mask NIV or switch to a helmet for NIV support for a planned enrollment of 206 patients (103 patients per group). The helmet is a transparent hood that covers the entire head of the patient and has a rubber collar neck seal. Early trial termination resulted in 44 patients randomized to the helmet group and 39 to the face mask group.
Main outcomes and measures: The primary outcome was the proportion of patients who required endotracheal intubation. Secondary outcomes included 28-day invasive ventilator-free days (ie, days alive without mechanical ventilation), duration of ICU and hospital length of stay, and hospital and 90-day mortality.
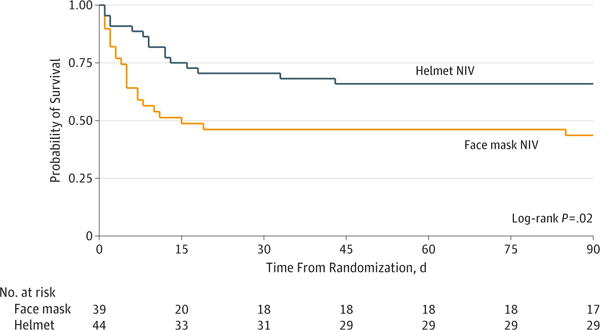
Results: Eighty-three patients (45% women; median age, 59 years; median Acute Physiology and Chronic Health Evaluation [APACHE] II score, 26) were included in the analysis after the trial was stopped early based on predefined criteria for efficacy. The intubation rate was 61.5% (n = 24) for the face mask group and 18.2% (n = 8) for the helmet group (absolute difference, -43.3%; 95% CI, -62.4% to -24.3%; P < .001). The number of ventilator-free days was significantly higher in the helmet group (28 vs 12.5, P < .001). At 90 days, 15 patients (34.1%) in the helmet group died compared with 22 patients (56.4%) in the face mask group (absolute difference, -22.3%; 95% CI, -43.3 to -1.4; P = .02). Adverse events included 3 interface-related skin ulcers for each group (ie, 7.6% in the face mask group had nose ulcers and 6.8% in the helmet group had neck ulcers).
Conclusions and relevance: Among patients with ARDS, treatment with helmet NIV resulted in a significant reduction of intubation rates. There was also a statistically significant reduction in 90-day mortality with helmet NIV. Multicenter studies are needed to replicate these findings.
Trial registration: clinicaltrials.gov Identifier: NCT01680783.
Conflict of interest statement
Figures
Comment in
-
Unmasking a Role for Noninvasive Ventilation in Early Acute Respiratory Distress Syndrome.JAMA. 2016 Jun 14;315(22):2401-3. doi: 10.1001/jama.2016.5987. JAMA. 2016. PMID: 27179463 Free PMC article. No abstract available.
-
Face Mask vs Helmet for Noninvasive Ventilation.JAMA. 2016 Oct 11;316(14):1496-1497. doi: 10.1001/jama.2016.13843. JAMA. 2016. PMID: 27727377 No abstract available.
-
Face Mask vs Helmet for Noninvasive Ventilation.JAMA. 2016 Oct 11;316(14):1496. doi: 10.1001/jama.2016.13852. JAMA. 2016. PMID: 27727378 No abstract available.
-
Non-invasive mechanical ventilation in hypoxemic respiratory failure: Just a matter of the interface?J Thorac Dis. 2016 Sep;8(9):2348-2352. doi: 10.21037/jtd.2016.08.43. J Thorac Dis. 2016. PMID: 27746973 Free PMC article. No abstract available.
-
Noninvasive ventilation for acute respiratory distress syndrome: the importance of ventilator settings.J Thorac Dis. 2016 Sep;8(9):E982-E986. doi: 10.21037/jtd.2016.09.29. J Thorac Dis. 2016. PMID: 27747041 Free PMC article.
-
A new horizon for the use of non-invasive ventilation in patients with acute respiratory distress syndrome.Ann Transl Med. 2016 Sep;4(18):348. doi: 10.21037/atm.2016.09.17. Ann Transl Med. 2016. PMID: 27761452 Free PMC article.
-
Non-invasive ventilation in acute respiratory distress syndrome: helmet use saves lives?Ann Transl Med. 2016 Sep;4(18):349. doi: 10.21037/atm.2016.08.09. Ann Transl Med. 2016. PMID: 27761453 Free PMC article. No abstract available.
-
Noninvasive ventilatory management of the acute respiratory distress syndrome: a new era or just another tease!Ann Transl Med. 2016 Sep;4(18):350. doi: 10.21037/atm.2016.08.38. Ann Transl Med. 2016. PMID: 27761454 Free PMC article. No abstract available.
-
Should we carry out noninvasive ventilation using a helmet in acute respiratory distress syndrome?Ann Transl Med. 2016 Sep;4(18):351. doi: 10.21037/atm.2016.08.35. Ann Transl Med. 2016. PMID: 27761455 Free PMC article. No abstract available.
-
Non-invasive ventilation in hypoxemic patients: does the interface make a difference?Ann Transl Med. 2016 Sep;4(18):359. doi: 10.21037/atm.2016.09.20. Ann Transl Med. 2016. PMID: 27761463 Free PMC article. No abstract available.
-
What's New in Noninvasive Ventilation: Factors Associated with Failure, Patterns of Use in Acute Asthma, and the Role of New Interfaces.Am J Respir Crit Care Med. 2017 Aug 15;196(4):520-522. doi: 10.1164/rccm.201609-1801RR. Am J Respir Crit Care Med. 2017. PMID: 28598218 No abstract available.
-
Helmet trials: resolving the puzzle.Intensive Care Med. 2023 Apr;49(4):458-461. doi: 10.1007/s00134-023-07004-z. Epub 2023 Mar 1. Intensive Care Med. 2023. PMID: 36856774 Free PMC article. No abstract available.
-
Personalized noninvasive respiratory support for acute hypoxemic respiratory failure.Intensive Care Med. 2023 Jul;49(7):840-843. doi: 10.1007/s00134-023-07048-1. Epub 2023 Apr 28. Intensive Care Med. 2023. PMID: 37115260 Free PMC article. No abstract available.
References
-
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416. - PubMed
-
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342(20):1471–1477. - PubMed
-
- Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291(14):1753–1762. - PubMed
-
- Kress JP, Hall JB. ICU-acquired weakness and recovery from critical illness. N Engl J Med. 2014;370(17):1626–1635. - PubMed
-
- Slutsky AS. Neuromuscular blocking agents in ARDS. N Engl J Med. 2010;363(12):1176–1180. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
