

Performance of ACMG-AMP Variant-Interpretation Guidelines among Nine Laboratories in the Clinical Sequencing Exploratory Research Consortium
- PMID: 27181684
- PMCID: PMC4908185
- DOI: 10.1016/j.ajhg.2016.03.024
Performance of ACMG-AMP Variant-Interpretation Guidelines among Nine Laboratories in the Clinical Sequencing Exploratory Research Consortium
Erratum in
-
Performance of ACMG-AMP Variant-Interpretation Guidelines among Nine Laboratories in the Clinical Sequencing Exploratory Research Consortium.Am J Hum Genet. 2016 Jul 7;99(1):247. doi: 10.1016/j.ajhg.2016.06.001. Am J Hum Genet. 2016. PMID: 27392081 Free PMC article. No abstract available.
Abstract
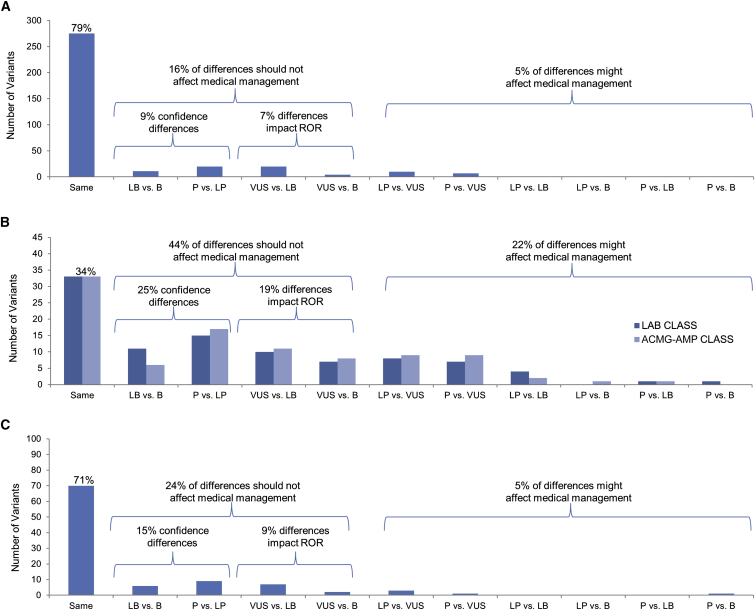
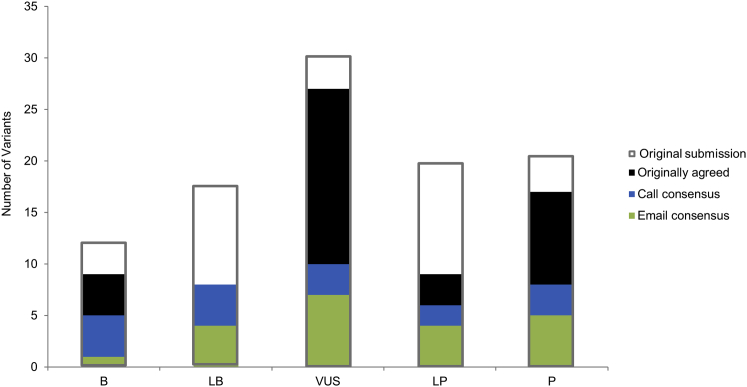
Evaluating the pathogenicity of a variant is challenging given the plethora of types of genetic evidence that laboratories consider. Deciding how to weigh each type of evidence is difficult, and standards have been needed. In 2015, the American College of Medical Genetics and Genomics (ACMG) and the Association for Molecular Pathology (AMP) published guidelines for the assessment of variants in genes associated with Mendelian diseases. Nine molecular diagnostic laboratories involved in the Clinical Sequencing Exploratory Research (CSER) consortium piloted these guidelines on 99 variants spanning all categories (pathogenic, likely pathogenic, uncertain significance, likely benign, and benign). Nine variants were distributed to all laboratories, and the remaining 90 were evaluated by three laboratories. The laboratories classified each variant by using both the laboratory's own method and the ACMG-AMP criteria. The agreement between the two methods used within laboratories was high (K-alpha = 0.91) with 79% concordance. However, there was only 34% concordance for either classification system across laboratories. After consensus discussions and detailed review of the ACMG-AMP criteria, concordance increased to 71%. Causes of initial discordance in ACMG-AMP classifications were identified, and recommendations on clarification and increased specification of the ACMG-AMP criteria were made. In summary, although an initial pilot of the ACMG-AMP guidelines did not lead to increased concordance in variant interpretation, comparing variant interpretations to identify differences and having a common framework to facilitate resolution of those differences were beneficial for improving agreement, allowing iterative movement toward increased reporting consistency for variants in genes associated with monogenic disease.
Copyright © 2016 American Society of Human Genetics. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Yorczyk A., Robinson L.S., Ross T.S. Use of panel tests in place of single gene tests in the cancer genetics clinic. Clin. Genet. 2015;88:278–282. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 HG006600/HG/NHGRI NIH HHS/United States
- R01 HG004500/HG/NHGRI NIH HHS/United States
- R21 HG006612/HG/NHGRI NIH HHS/United States
- R21 HG006613/HG/NHGRI NIH HHS/United States
- U01 HG008657/HG/NHGRI NIH HHS/United States
- R21 HG006596/HG/NHGRI NIH HHS/United States
- U41 HG006834/HG/NHGRI NIH HHS/United States
- R01 HG006615/HG/NHGRI NIH HHS/United States
- U01 HG006507/HG/NHGRI NIH HHS/United States
- U01 HG006485/HG/NHGRI NIH HHS/United States
- R01 HG006618/HG/NHGRI NIH HHS/United States
- U01 HG006500/HG/NHGRI NIH HHS/United States
- RM1 HG007257/HG/NHGRI NIH HHS/United States
- R21 HG006594/HG/NHGRI NIH HHS/United States
- UM1 HG007301/HG/NHGRI NIH HHS/United States
- U01 HG007307/HG/NHGRI NIH HHS/United States
- UM1 HG006508/HG/NHGRI NIH HHS/United States
- U01 HG006546/HG/NHGRI NIH HHS/United States
- P50 HG007257/HG/NHGRI NIH HHS/United States
- U01 HG007292/HG/NHGRI NIH HHS/United States
- UM1 HG007292/HG/NHGRI NIH HHS/United States
- R01 CA154517/CA/NCI NIH HHS/United States
- U01 HG006487/HG/NHGRI NIH HHS/United States
- U01 HG006492/HG/NHGRI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
