

Pseudo-Meigs' syndrome secondary to metachronous ovarian metastases from transverse colon cancer
- PMID: 27182170
- PMCID: PMC4858642
- DOI: 10.3748/wjg.v22.i18.4604
Pseudo-Meigs' syndrome secondary to metachronous ovarian metastases from transverse colon cancer
Abstract
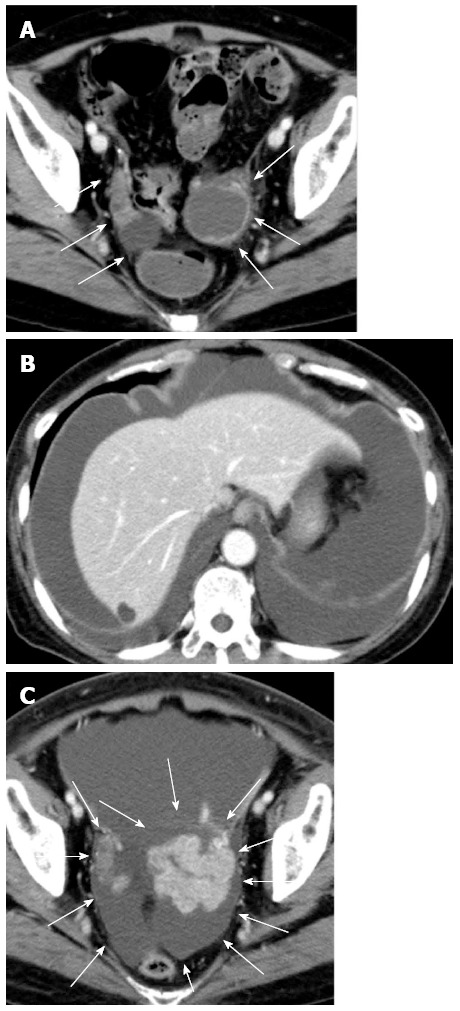
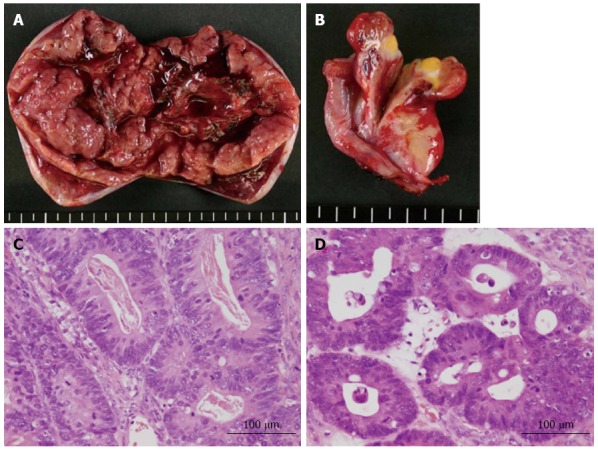
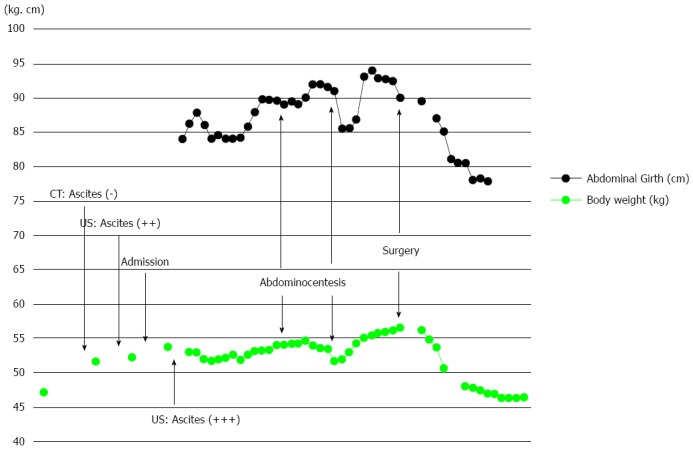
Pseudo-Meigs' syndrome associated with colorectal cancer is extremely rare. We report here a case of pseudo-Meigs' syndrome secondary to metachronous ovarian metastases from colon cancer. A 65-year-old female with a history of surgery for transverse colon cancer and peritoneal dissemination suffered from metachronous ovarian metastases during treatment with systemic chemotherapy. At first, neither ascites nor pleural effusion was observed, but she later complained of progressive abdominal distention and dyspnea caused by rapidly increasing ascites and pleural effusion and rapidly enlarging ovarian metastases. Abdominocenteses were repeated, and cytological examinations of the fluids were all negative for malignant cells. We suspected pseudo-Meigs' syndrome, and bilateral oophorectomies were performed after thorough informed consent. The patient's postoperative condition improved rapidly after surgery. We conclude that pseudo-Meigs' syndrome should be included in the differential diagnosis of massive or rapidly increasing ascites and pleural effusion associated with large or rapidly enlarging ovarian tumors.
Keywords: Ascites; Colon cancer; Ovarian metastasis; Pleural effusion; Pseudo-Meigs’ syndrome.
Figures
Similar articles
-
Long-term survival in pseudo-Meigs' syndrome caused by ovarian metastases from colon cancer.World J Surg Oncol. 2016 Nov 14;14(1):286. doi: 10.1186/s12957-016-1040-0. World J Surg Oncol. 2016. PMID: 27842595 Free PMC article.
-
Pseudo-Meigs' syndrome caused by ovarian metastasis from colon cancer: report of a case.Surg Today. 2003;33(5):387-91. doi: 10.1007/s005950300088. Surg Today. 2003. PMID: 12734738
-
Pseudo-Meigs' syndrome caused by secondary ovarian tumors from gastrointestinal cancer. A case report and review of the literature.Dig Surg. 2000;17(4):418-9. doi: 10.1159/000018893. Dig Surg. 2000. PMID: 11053957 Review.
-
VEGF hypersecretion as a plausible mechanism for pseudo-meigs' syndrome in advanced colorectal cancer.Jpn J Clin Oncol. 2010 May;40(5):476-81. doi: 10.1093/jjco/hyq014. Epub 2010 Feb 23. Jpn J Clin Oncol. 2010. PMID: 20181551
-
Pseudo-Meigs' syndrome secondary to isolated colorectal metastasis to ovary: a case report and review of the literature.Gynecol Oncol. 2004 Apr;93(1):248-51. doi: 10.1016/j.ygyno.2003.12.025. Gynecol Oncol. 2004. PMID: 15047245 Review.
Cited by
-
SNP rs12982687 affects binding capacity of lncRNA UCA1 with miR-873-5p: involvement in smoking-triggered colorectal cancer progression.Cell Commun Signal. 2020 Mar 6;18(1):37. doi: 10.1186/s12964-020-0518-0. Cell Commun Signal. 2020. PMID: 32143722 Free PMC article.
-
Atypical Pseudo-Meigs' Syndrome without Pleural Effusion Due to Ovarian Metastasis from Sigmoid Colon Cancer.Intern Med. 2023 May 15;62(10):1487-1493. doi: 10.2169/internalmedicine.0157-22. Epub 2022 Oct 12. Intern Med. 2023. PMID: 36223922 Free PMC article.
-
Abdominopelvic leiomyoma with large ascites: A case report and review of the literature.World J Clin Cases. 2021 Feb 26;9(6):1424-1432. doi: 10.12998/wjcc.v9.i6.1424. World J Clin Cases. 2021. PMID: 33644211 Free PMC article.
References
-
- Meigs JV, Cass JW. Fibroma of the ovary with ascites and hydrothorax: a report of seven cases. Am J Obstet Gynecol. 1937;33:249–266.
-
- Meigs JV. Pelvic tumors other than fibromas of the ovary with ascites and hydrothorax. Obstet Gynecol. 1954;3:471–486. - PubMed
-
- Rhoads JE, Terrell AW. Ovarian fibroma with ascites and hydrothorax (Meigs’ syndrome) JAMA. 1937;109:1684–1687.
-
- Ryan RJ. PseudoMeigs syndrome. Associated with metastatic cancer of ovary. N Y State J Med. 1972;72:727–730. - PubMed
-
- Matsuzaki M, Murase M, Kamiya I, Horio S, Sakuma H. A case of Meigs’ syndrome resulting from rectal cancer (in Japanese with English abstract) J Jpn Soc Clin Surg. 1992;53:667–670.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
