

White matter microstructural changes in adolescent anorexia nervosa including an exploratory longitudinal study
- PMID: 27182488
- PMCID: PMC4857215
- DOI: 10.1016/j.nicl.2016.04.002
White matter microstructural changes in adolescent anorexia nervosa including an exploratory longitudinal study
Abstract
Background: Anorexia nervosa (AN) often begins in adolescence, however, the understanding of the underlying pathophysiology at this developmentally important age is scarce, impeding early interventions. We used diffusion tensor imaging (DTI) to investigate microstructural white matter (WM) brain changes including an experimental longitudinal follow-up.
Methods: We acquired whole brain diffusion-weighted brain scans of 22 adolescent female hospitalized patients with AN at admission and nine patients longitudinally at discharge after weight rehabilitation. Patients (10-18 years) were compared to 21 typically developing controls (TD). Tract-based spatial statistics (TBSS) were applied to compare fractional anisotropy (FA) across groups and time points. Associations between average FA values of the global WM skeleton and weight as well as illness duration parameters were analyzed by multiple linear regression.
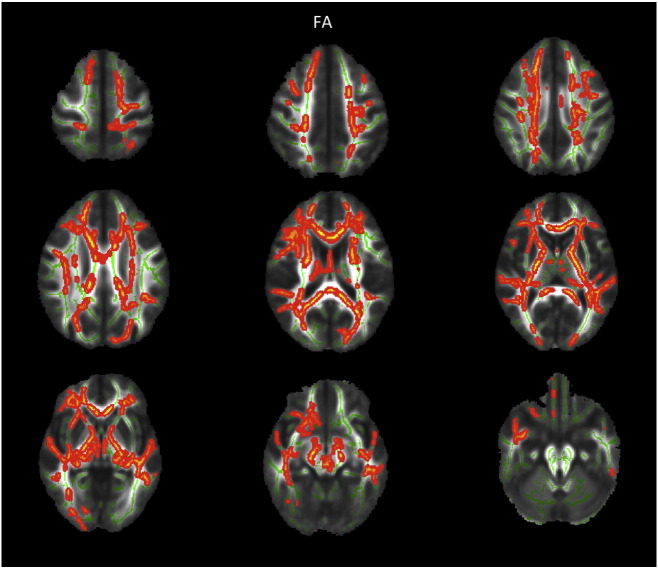
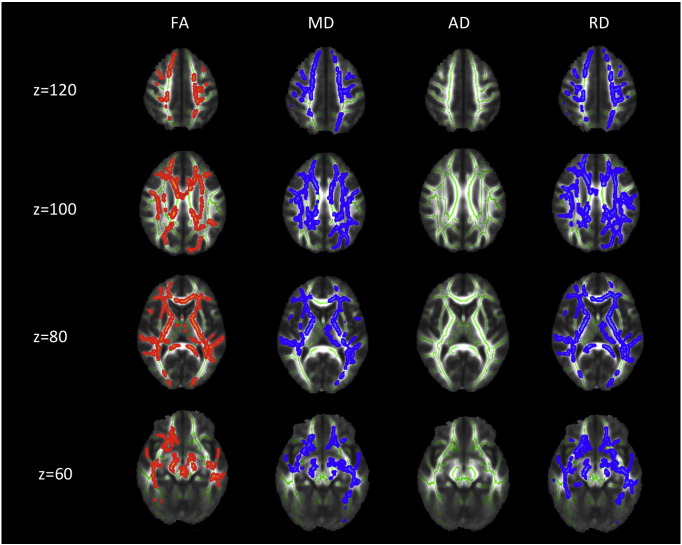
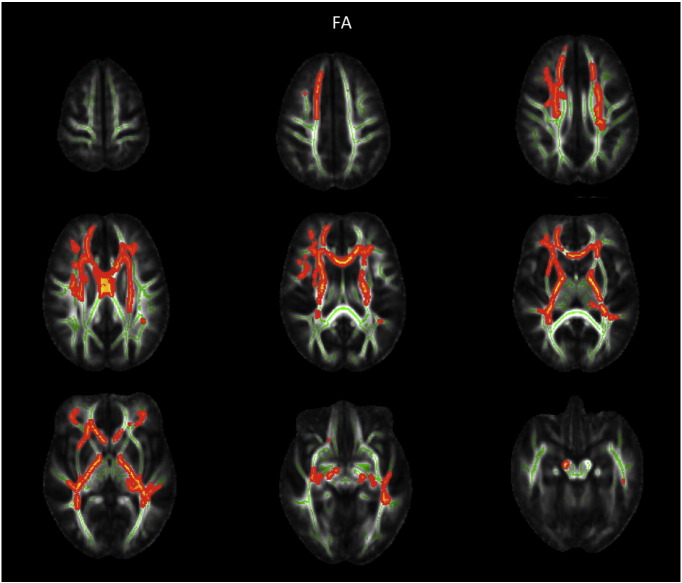
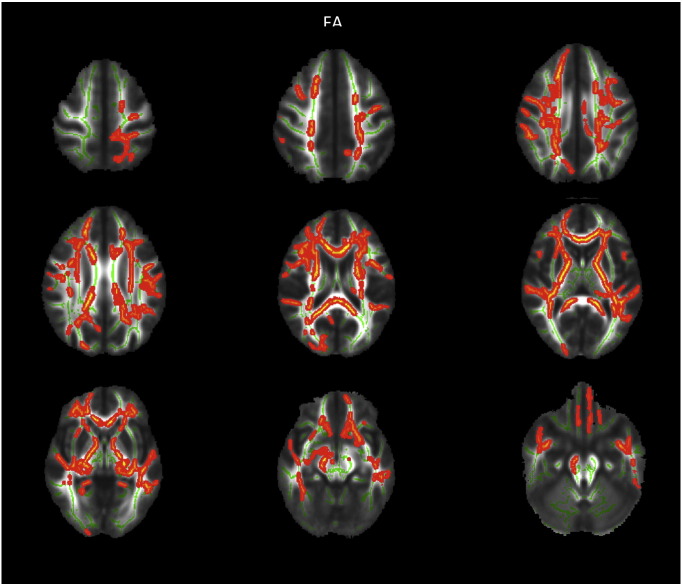
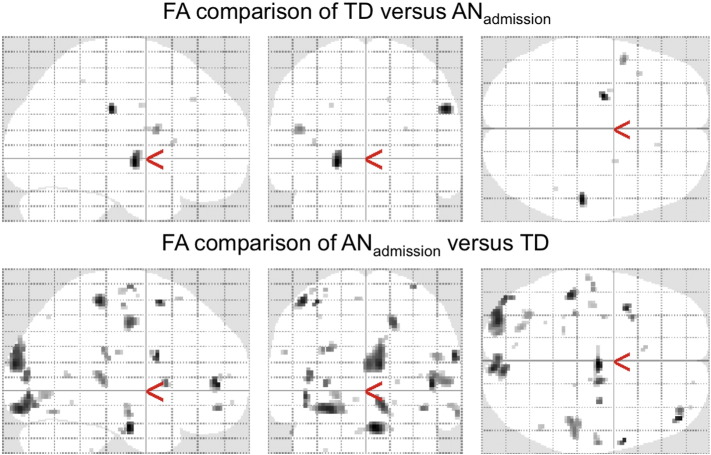
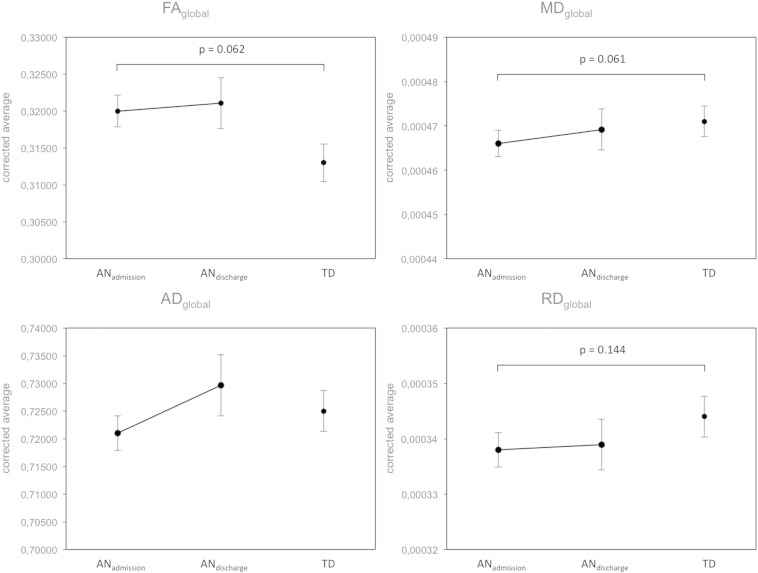
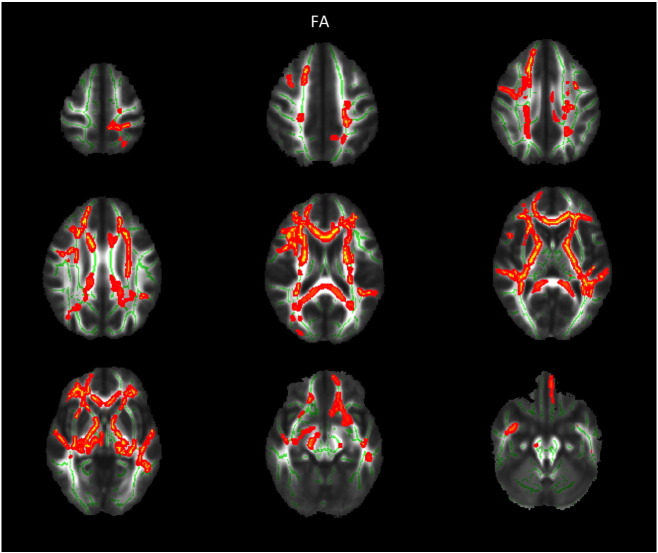
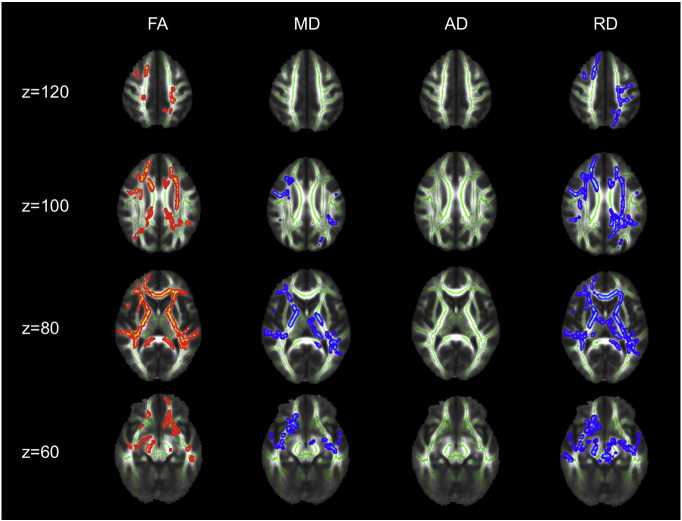
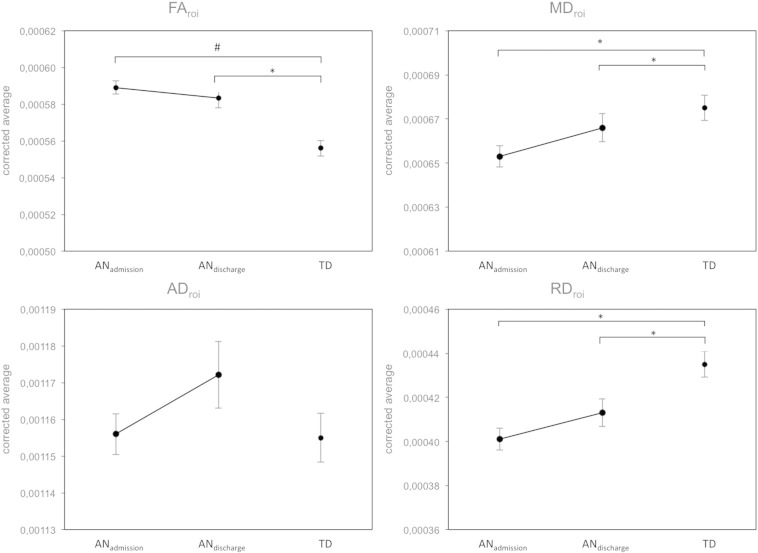
Results: We observed increased FA in bilateral frontal, parietal and temporal areas in AN patients at admission compared to TD. Higher FA of the global WM skeleton at admission was associated with faster weight loss prior to admission. Exploratory longitudinal analysis showed this FA increase to be partially normalized after weight rehabilitation.
Conclusions: Our findings reveal a markedly different pattern of WM microstructural changes in adolescent AN compared to most previous results in adult AN. This could signify a different susceptibility and reaction to semi-starvation in the still developing brain of adolescents or a time-dependent pathomechanism differing with extend of chronicity. Higher FA at admission in adolescents with AN could point to WM fibers being packed together more closely.
Keywords: Adolescence; Anorexia nervosa; DTI; Fractional anisotropy; TBSS.
Figures
Similar articles
-
Developmental stage-dependent relationships between ghrelin levels and hippocampal white matter connections in low-weight anorexia nervosa and atypical anorexia nervosa.Psychoneuroendocrinology. 2020 Sep;119:104722. doi: 10.1016/j.psyneuen.2020.104722. Epub 2020 May 23. Psychoneuroendocrinology. 2020. PMID: 32512249 Free PMC article.
-
Dynamic changes in white matter microstructure in anorexia nervosa: findings from a longitudinal study.Psychol Med. 2019 Jul;49(9):1555-1564. doi: 10.1017/S003329171800212X. Epub 2018 Aug 28. Psychol Med. 2019. PMID: 30149815
-
Disruption of brain white matter microstructure in women with anorexia nervosa.J Psychiatry Neurosci. 2014 Nov;39(6):367-75. doi: 10.1503/jpn.130135. J Psychiatry Neurosci. 2014. PMID: 24913136 Free PMC article.
-
White matter alterations in anorexia nervosa: Evidence from a voxel-based meta-analysis.Neurosci Biobehav Rev. 2019 May;100:285-295. doi: 10.1016/j.neubiorev.2019.03.002. Epub 2019 Mar 6. Neurosci Biobehav Rev. 2019. PMID: 30851283 Review.
-
Altered thalamo–cortical and occipital–parietal– temporal–frontal white matter connections in patients with anorexia and bulimia nervosa: a systematic review of diffusion tensor imaging studies.J Psychiatry Neurosci. 2019 Sep 1;44(5):324-339. doi: 10.1503/jpn.180121. J Psychiatry Neurosci. 2019. PMID: 30994310 Free PMC article.
Cited by
-
Structural Neuroimaging of Anorexia Nervosa: Future Directions in the Quest for Mechanisms Underlying Dynamic Alterations.Biol Psychiatry. 2018 Feb 1;83(3):224-234. doi: 10.1016/j.biopsych.2017.08.011. Epub 2017 Aug 24. Biol Psychiatry. 2018. PMID: 28967386 Free PMC article. Review.
-
White Matter Abnormalities in the Corpus Callosum in Acute and Recovered Anorexia Nervosa Patients-A Diffusion Tensor Imaging Study.Front Psychiatry. 2019 Jul 8;10:490. doi: 10.3389/fpsyt.2019.00490. eCollection 2019. Front Psychiatry. 2019. PMID: 31338044 Free PMC article.
-
Limbic-thalamo-cortical projections and reward-related circuitry integrity affects eating behavior: A longitudinal DTI study in adolescents with restrictive eating disorders.PLoS One. 2017 Mar 1;12(3):e0172129. doi: 10.1371/journal.pone.0172129. eCollection 2017. PLoS One. 2017. PMID: 28248991 Free PMC article. Clinical Trial.
-
Extend, Pathomechanism and Clinical Consequences of Brain Volume Changes in Anorexia Nervosa.Curr Neuropharmacol. 2018;16(8):1164-1173. doi: 10.2174/1570159X15666171109145651. Curr Neuropharmacol. 2018. PMID: 29119931 Free PMC article. Review.
-
Developmental stage-dependent relationships between ghrelin levels and hippocampal white matter connections in low-weight anorexia nervosa and atypical anorexia nervosa.Psychoneuroendocrinology. 2020 Sep;119:104722. doi: 10.1016/j.psyneuen.2020.104722. Epub 2020 May 23. Psychoneuroendocrinology. 2020. PMID: 32512249 Free PMC article.
References
-
- American Psychiatric Association, editor. Diagnostic and Statistical Manual of Mental Disorders DSM-5. 5. ed. American Psychiatric Publishing; Washington, DC: 2013. (u.a.)
-
- Andersson J.L.R., Skare S., Ashburner J. How to correct susceptibility distortions in spin-echo echo-planar images: application to diffusion tensor imaging. NeuroImage. 2003;20:870–888. - PubMed
-
- Bach M., Laun F.B., Leemans A., Tax C.M.W., Biessels G.J., Stieltjes B., Maier-Hein K.H. Methodological considerations on tract-based spatial statistics (TBSS) NeuroImage. 2014;100:358–369. - PubMed
-
- Bazarian J.J., Zhong J., Blyth B., Zhu T., Kavcic V., Peterson D. Diffusion tensor imaging detects clinically important axonal damage after mild traumatic brain injury: a pilot study. J. Neurotrauma. 2007;24:1447–1459. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
