

The Correlation of Skeletal and Cardiac Muscle Dysfunction in Duchenne Muscular Dystrophy
- PMID: 27182492
- PMCID: PMC4864001
- DOI: 10.3233/JND-150132
The Correlation of Skeletal and Cardiac Muscle Dysfunction in Duchenne Muscular Dystrophy
Abstract
Background: Duchenne muscular dystrophy (DMD) is characterized by progressive skeletal muscle and cardiac dysfunction. While skeletal muscle dysfunction precedes cardiomyopathy, the relationship between the progressive decline in skeletal and cardiac muscle function is unclear. This relationship is especially important given that the myocardial effects of many developing DMD therapies are largely unknown.
Objective: Our objective was to assess the relationship between progression of skeletal muscle weakness and onset of cardiac dysfunction in DMD.
Methods: A total of 77 DMD subjects treated at a single referral center were included. Demographic information, quantitative muscle testing (QMT), subjective muscle strength, cardiac function, and current and retrospective medications were collected. A Spearman rank correlation was used to evaluate for an association between subjective strength and fractional shortening. The effects of total QMT and arm QMT on fractional shortening were examined in generalized least square with and without adjustments for age, ambulatory status, and duration of corticosteroids and cardiac specific medications.
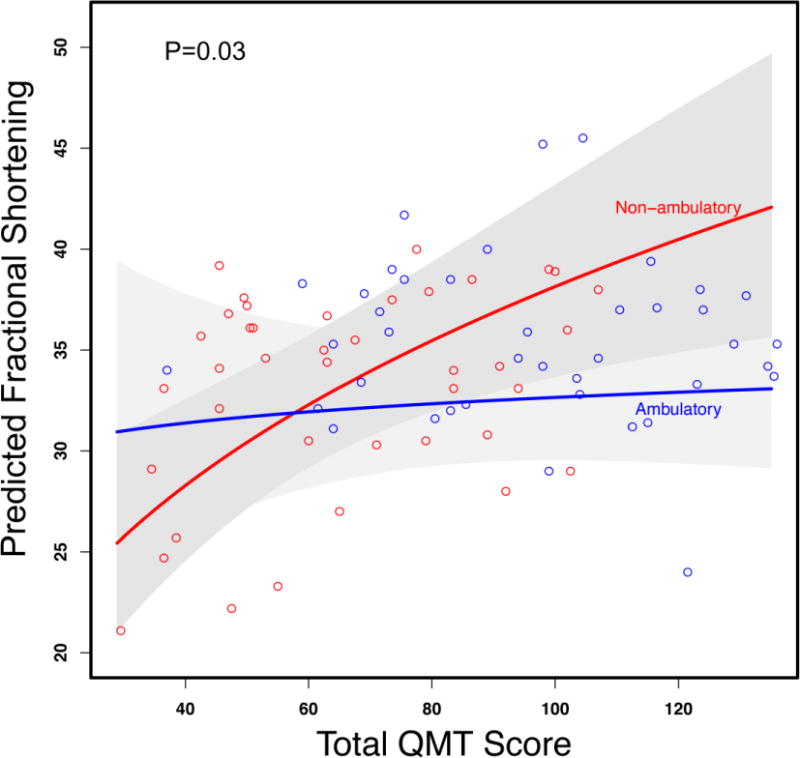
Results: We found a significant correlation between maintained subjective skeletal muscle arm and leg strength and maintained cardiac function as defined by fractional shortening (rho=0.47, p=0.004 and rho=0.48, p=0.003, respectively). We also found a significant association between QMT and fractional shortening among non-ambulatory DMD subjects (p=0.03), while this association was not significant in ambulatory subjects.
Conclusions: Our findings allow us to conclude that in this population, there exists a significant relationship between skeletal muscle and cardiac function in non-ambulatory DMD patients. While this does not imply a causal relationship, a possible association between skeletal and cardiac muscle function suggests that researchers should carefully monitor cardiac function, even when the primary outcome measures are not cardiac in nature.
Keywords: Ambulation; Cardiac dysfunction; Cardiomyopathy; Duchenne muscular dystrophy; Skeletal muscle dysfunction.
Conflict of interest statement
The authors have no conflict of interest to report.
Figures
References
-
- Dooley J, Gordon KE, Dodds L, MacSween J. Duchenne muscular dystrophy: a 30-year population-based incidence study. Clin Pediatr (Phila) 2010;49(2):177–9. - PubMed
-
- Hoffman EP, Brown RH, Jr, Kunkel LM. Dystrophin: the protein product of the Duchenne muscular dystrophy locus. Cell. 1987;51(6):919–28. - PubMed
-
- Boland BJ, Silbert PL, Groover RV, Wollan PC, Silverstein MD. Skeletal, cardiac, and smooth muscle failure in Duchenne muscular dystrophy. Pediatr Neurol. 1996;14(1):7–12. - PubMed
-
- Nigro G, Comi LI, Politano L, Bain RJ. The incidence and evolution of cardiomyopathy in Duchenne muscular dystrophy. International journal of cardiology. 1990;26(3):271–7. - PubMed
-
- Eagle M, Baudouin SV, Chandler C, Giddings DR, Bullock R, Bushby K. Survival in Duchenne muscular dystrophy: improvements in life expectancy since 1967 and the impact of home nocturnal ventilation. Neuromuscul Disord. 2002;12(10):926–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
