

Antibiotic Prescriptions and Prophylaxis in Italian Children. Is It Time to Change? Data from the ARPEC Project
- PMID: 27182926
- PMCID: PMC4868290
- DOI: 10.1371/journal.pone.0154662
Antibiotic Prescriptions and Prophylaxis in Italian Children. Is It Time to Change? Data from the ARPEC Project
Abstract
Background: Antimicrobials are the most commonly prescribed drugs. Many studies have evaluated antibiotic prescriptions in the paediatric outpatient but few studies describing the real antibiotic consumption in Italian children's hospitals have been published. Point-prevalence survey (PPS) has been shown to be a simple, feasible and reliable standardized method for antimicrobials surveillance in children and neonates admitted to the hospital. In this paper, we presented data from a PPS on antimicrobial prescriptions carried out in 7 large Italian paediatric institutions.
Methods: A 1-day PPS on antibiotic use in hospitalized neonates and children was performed in Italy between October and December 2012 as part of the Antibiotic Resistance and Prescribing in European Children project (ARPEC). Seven institutions in seven Italian cities were involved. The survey included all admitted patients less than 18 years of age present in the ward at 8:00 am on the day of the survey, who had at least one on-going antibiotic prescription. For all patients data about age, weight, underlying disease, antimicrobial agent, dose and indication for treatment were collected.
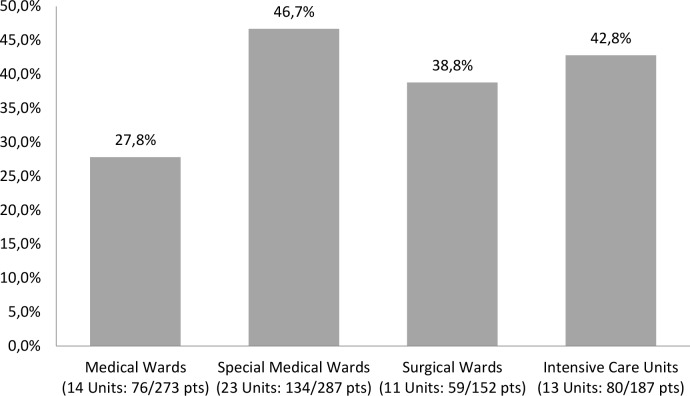
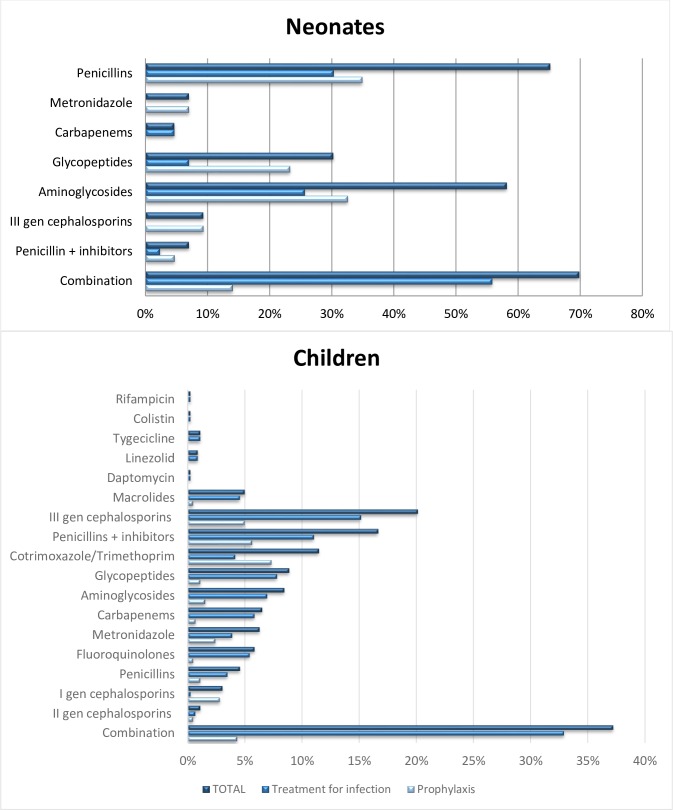
Results: The PPS was performed in 61 wards within 7 Italian institutions. A total of 899 patients were eligible and 349 (38.9%) had an on-going prescription for one or more antibiotics, with variable rates among the hospitals (25.7% - 53.8%). We describe antibiotic prescriptions separately in neonates (<30 days old) and children (> = 30 days to <18 years old). In the neonatal cohort, 62.8% received antibiotics for prophylaxis and only 37.2% on those on antibiotics were treated for infection. Penicillins and aminoglycosides were the most prescribed antibiotic classes. In the paediatric cohort, 64.4% of patients were receiving antibiotics for treatment of infections and 35.5% for prophylaxis. Third generation cephalosporins and penicillin plus inhibitors were the top two antibiotic classes. The main reason for prescribing antibiotic therapy in children was lower respiratory tract infections (LRTI), followed by febrile neutropenia/fever in oncologic patients, while, in neonates, sepsis was the most common indication for treatment. Focusing on prescriptions for LRTI, 43.3% of patients were treated with 3rd generation cephalosporins, followed by macrolides (26.9%), quinolones (16.4%) and carbapenems (14.9%) and 50.1% of LRTI cases were receiving more than one antibiotic. For neutropenic fever/fever in oncologic patients, the preferred antibiotics were penicillins with inhibitors (47.8%), followed by carbapenems (34.8%), aminoglycosides (26.1%) and glycopeptides (26.1%). Overall, the 60.9% of patients were treated with a combination therapy.
Conclusions: Our study provides insight on the Italian situation in terms of antibiotic prescriptions in hospitalized neonates and children. An over-use of third generation cephalosporins both for prophylaxis and treatment was the most worrisome finding. A misuse and abuse of carbapenems and quinolones was also noted. Antibiotic stewardship programs should immediately identify feasible targets to monitor and modify the prescription patterns in children's hospital, also considering the continuous and alarming emergence of MDR bacteria.
Conflict of interest statement
Figures
References
-
- Van der Meer JW, Gyssens IC. Quality of antimicrobial drug prescription in hospital. Clin Microbiol Infect. 2001;7 Suppl 6:12–5. - PubMed
-
- CDC, Antibiotic Resistance Threats in the United States, 2013 available at www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf - PubMed
-
- Hecker MT, Aron DC, Patel NP, Lehmann MK, Donskey CJ. Unnecessary use of antimicrobials in hospitalized patients: current patterns of misuse with an emphasis on the antianaerobic spectrum of activity. Arch Intern Med. 2003;163(8):972–978. - PubMed
-
- Dellit TH, Owens RC, McGowan JE Jr, Gerding DN, Weinstein RA, Burke JP, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(2):159–177. - PubMed
-
- Cosgrove SE, Carmeli Y. The impact of antimicrobial resistance on health and economic outcomes. Clin Infect Dis. 2003;36(11):1433–1437. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
