

Comparative Effectiveness of Tai Chi Versus Physical Therapy for Knee Osteoarthritis: A Randomized Trial
- PMID: 27183035
- PMCID: PMC4960454
- DOI: 10.7326/M15-2143
Comparative Effectiveness of Tai Chi Versus Physical Therapy for Knee Osteoarthritis: A Randomized Trial
Abstract
Background: Few remedies effectively treat long-term pain and disability from knee osteoarthritis. Studies suggest that Tai Chi alleviates symptoms, but no trials have directly compared Tai Chi with standard therapies for osteoarthritis.
Objective: To compare Tai Chi with standard physical therapy for patients with knee osteoarthritis.
Design: Randomized, 52-week, single-blind comparative effectiveness trial. (ClinicalTrials.gov: NCT01258985).
Setting: An urban tertiary care academic hospital.
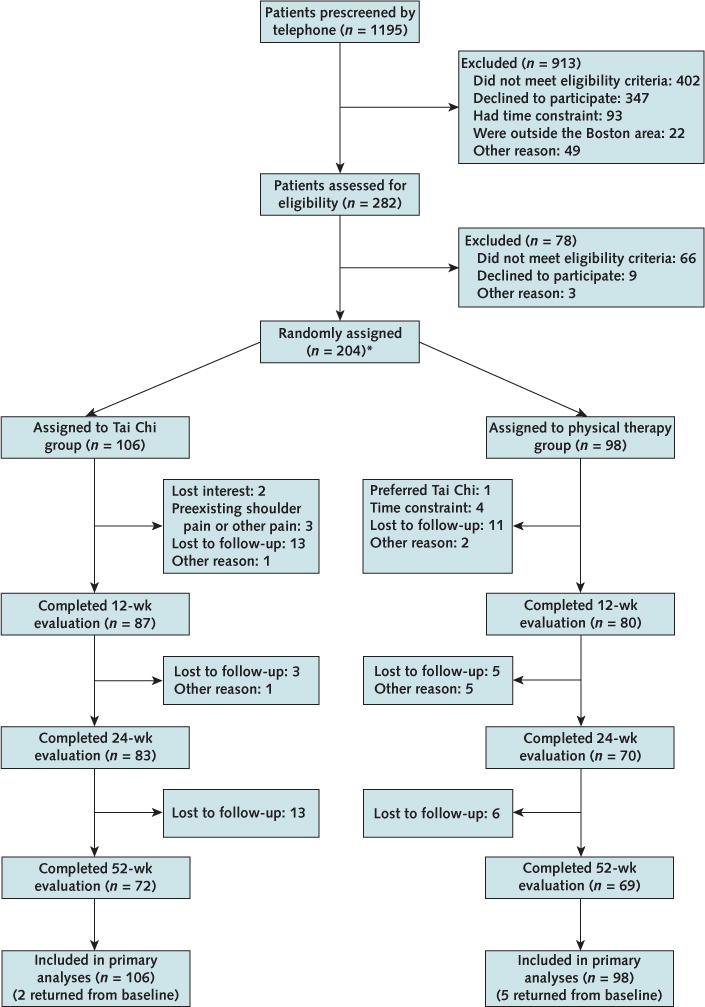
Patients: 204 participants with symptomatic knee osteoarthritis (mean age, 60 years; 70% women; 53% white).
Intervention: Tai Chi (2 times per week for 12 weeks) or standard physical therapy (2 times per week for 6 weeks, followed by 6 weeks of monitored home exercise).
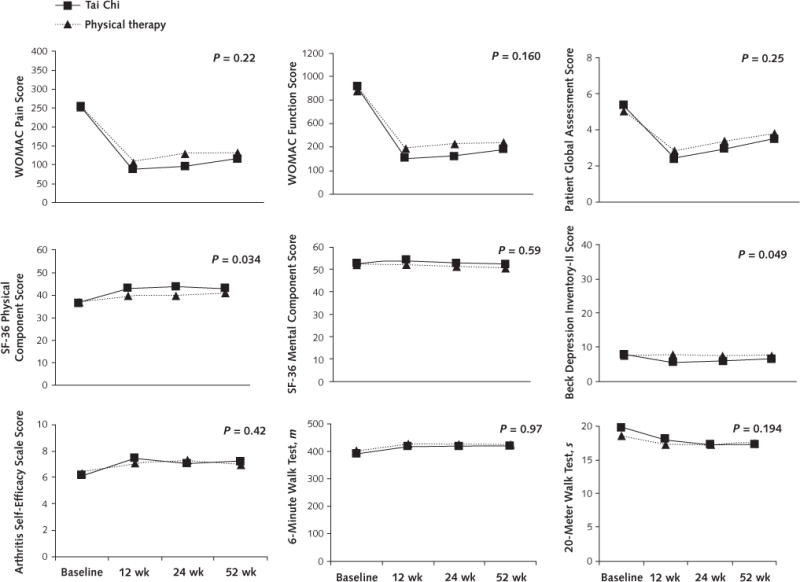
Measurements: The primary outcome was Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score at 12 weeks. Secondary outcomes included physical function, depression, medication use, and quality of life.
Results: At 12 weeks, the WOMAC score was substantially reduced in both groups (Tai Chi, 167 points [95% CI, 145 to 190 points]; physical therapy, 143 points [CI, 119 to 167 points]). The between-group difference was not significant (24 points [CI, -10 to 58 points]). Both groups also showed similar clinically significant improvement in most secondary outcomes, and the benefits were maintained up to 52 weeks. Of note, the Tai Chi group had significantly greater improvements in depression and the physical component of quality of life. The benefit of Tai Chi was consistent across instructors. No serious adverse events occurred.
Limitation: Patients were aware of their treatment group assignment, and the generalizability of the findings to other settings remains undetermined.
Conclusion: Tai Chi produced beneficial effects similar to those of a standard course of physical therapy in the treatment of knee osteoarthritis.
Primary funding source: National Center for Complementary and Integrative Health of the National Institutes of Health.
Conflict of interest statement
Figures
Comment in
-
Similar benefits from Tai Chi and supervised physiotherapy for knee osteoarthritis [commentary].J Physiother. 2017 Apr;63(2):116. doi: 10.1016/j.jphys.2017.02.011. Epub 2017 Feb 24. J Physiother. 2017. PMID: 28314648 No abstract available.
-
Similar benefits from Tai Chi and supervised physiotherapy for knee osteoarthritis [synopsis].J Physiother. 2017 Apr;63(2):116. doi: 10.1016/j.jphys.2017.02.005. Epub 2017 Feb 27. J Physiother. 2017. PMID: 28314649 No abstract available.
Summary for patients in
-
Tai Chi Versus Physical Therapy for Knee Osteoarthritis.Ann Intern Med. 2016 Jul 19;165(2). doi: 10.7326/P16-9017. Epub 2016 May 17. Ann Intern Med. 2016. PMID: 27183300 No abstract available.
References
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–223. doi: 10.1016/S0140-6736(12)61689-4. - DOI - PubMed
-
- Smalley WE, Griffin MR. The risks and costs of upper gastrointestinal disease attributable to NSAIDs. Gastroenterol Clin North Am. 1996;25:373–96. - PubMed
-
- Jamtvedt G, Dahm KT, Christie A, Moe RH, Haavardsholm E, Holm I, et al. Physical therapy interventions for patients with osteoarthritis of the knee: an overview of systematic reviews. Phys Ther. 2008;88:123–36. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical