

Ruling Out Pulmonary Embolism in Primary Care: Comparison of the Diagnostic Performance of "Gestalt" and the Wells Rule
- PMID: 27184993
- PMCID: PMC4868561
- DOI: 10.1370/afm.1930
Ruling Out Pulmonary Embolism in Primary Care: Comparison of the Diagnostic Performance of "Gestalt" and the Wells Rule
Abstract
Purpose: Diagnostic prediction models such as the Wells rule can be used for safely ruling out pulmonary embolism (PE) when it is suspected. A physician's own probability estimate ("gestalt"), however, is commonly used instead. We evaluated the diagnostic performance of both approaches in primary care.
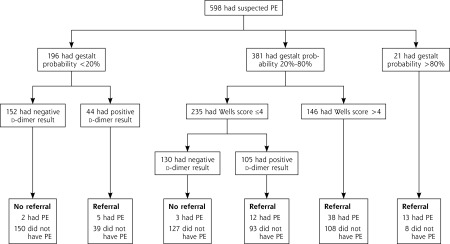
Methods: Family physicians estimated the probability of PE on a scale of 0% to 100% (gestalt) and calculated the Wells rule score in 598 patients with suspected PE who were thereafter referred to secondary care for definitive testing. We compared the discriminative ability (c statistic) of both approaches. Next, we stratified patients into PE risk categories. For gestalt, a probability of less than 20% plus a negative point-of-care d-dimer test indicated low risk; for the Wells rule, we used a score of 4 or lower plus a negative d-dimer test. We compared sensitivity, specificity, efficiency (percentage of low-risk patients in total cohort), and failure rate (percentage of patients having PE within the low-risk category).
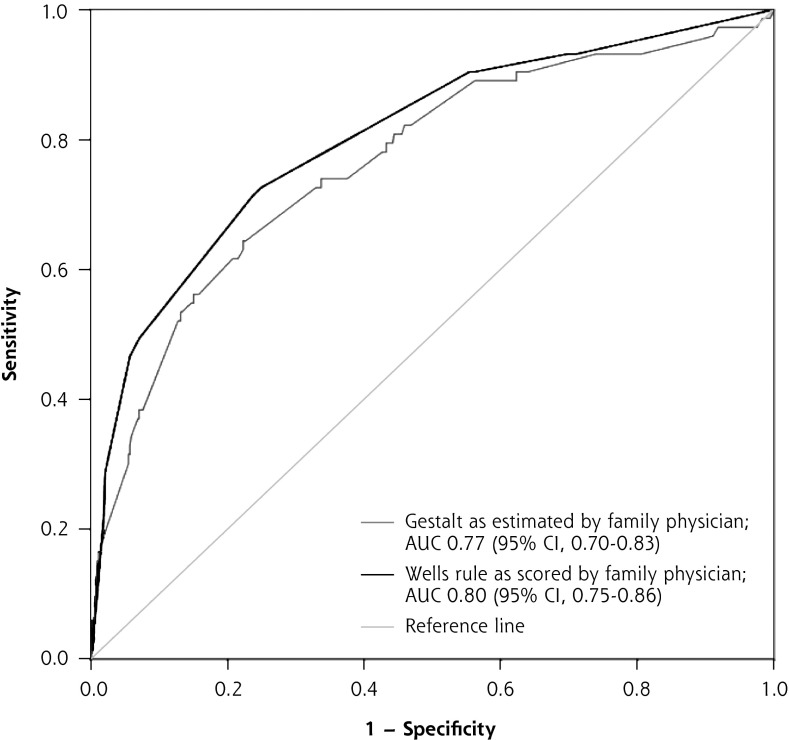
Results: With 3 months of follow-up, 73 patients (12%) were confirmed to have venous thromboembolism (a surrogate for PE at baseline). The c statistic was 0.77 (95% CI, 0.70-0.83) for gestalt and 0.80 (95% CI, 0.75-0.86) for the Wells rule. Gestalt missed 2 out of 152 low-risk patients (failure rate = 1.3%; 95% CI, 0.2%-4.7%) with an efficiency of 25% (95% CI, 22%-29%); the Wells rule missed 4 out of 272 low-risk patients (failure rate = 1.5%; 95% CI, 0.4%-3.7%) with an efficiency of 45% (95% CI, 41%-50%).
Conclusions: Combined with d-dimer testing, both gestalt using a cutoff of less than 20% and the Wells rule using a score of 4 or lower are safe for ruling out PE in primary care. The Wells rule is more efficient, however, and PE can be ruled out in a larger proportion of suspected cases.
Keywords: deep venous thrombosis; diagnostic prediction models; family practice; gestalt; practice-based research; primary care; pulmonary embolism.
© 2016 Annals of Family Medicine, Inc.
Figures

References
-
- PIOPED Investigators. Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED). JAMA. 1990;263(20): 2753–2759. - PubMed
-
- Konstantinides SV, Torbicki A, Agnelli G, et al. ; Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033–3069, 3069a–3069k. - PubMed
-
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED d-dimer. Thromb Haemost. 2000;83(3):416–420. - PubMed
-
- Le Gal G, Righini M, Roy P-M, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006;144(3):165–171. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical