

Rectal Cancer: Assessment of Neoadjuvant Chemoradiation Outcome based on Radiomics of Multiparametric MRI
- PMID: 27185368
- PMCID: PMC10916000
- DOI: 10.1158/1078-0432.CCR-15-2997
Rectal Cancer: Assessment of Neoadjuvant Chemoradiation Outcome based on Radiomics of Multiparametric MRI
Abstract
Purpose: To evaluate multiparametric MRI features in predicting pathologic response after preoperative chemoradiation therapy (CRT) for locally advanced rectal cancer (LARC).
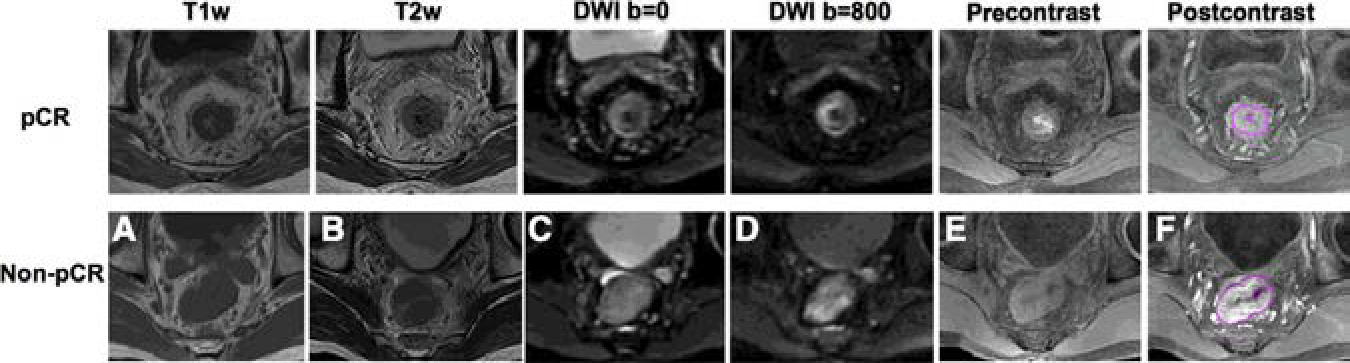
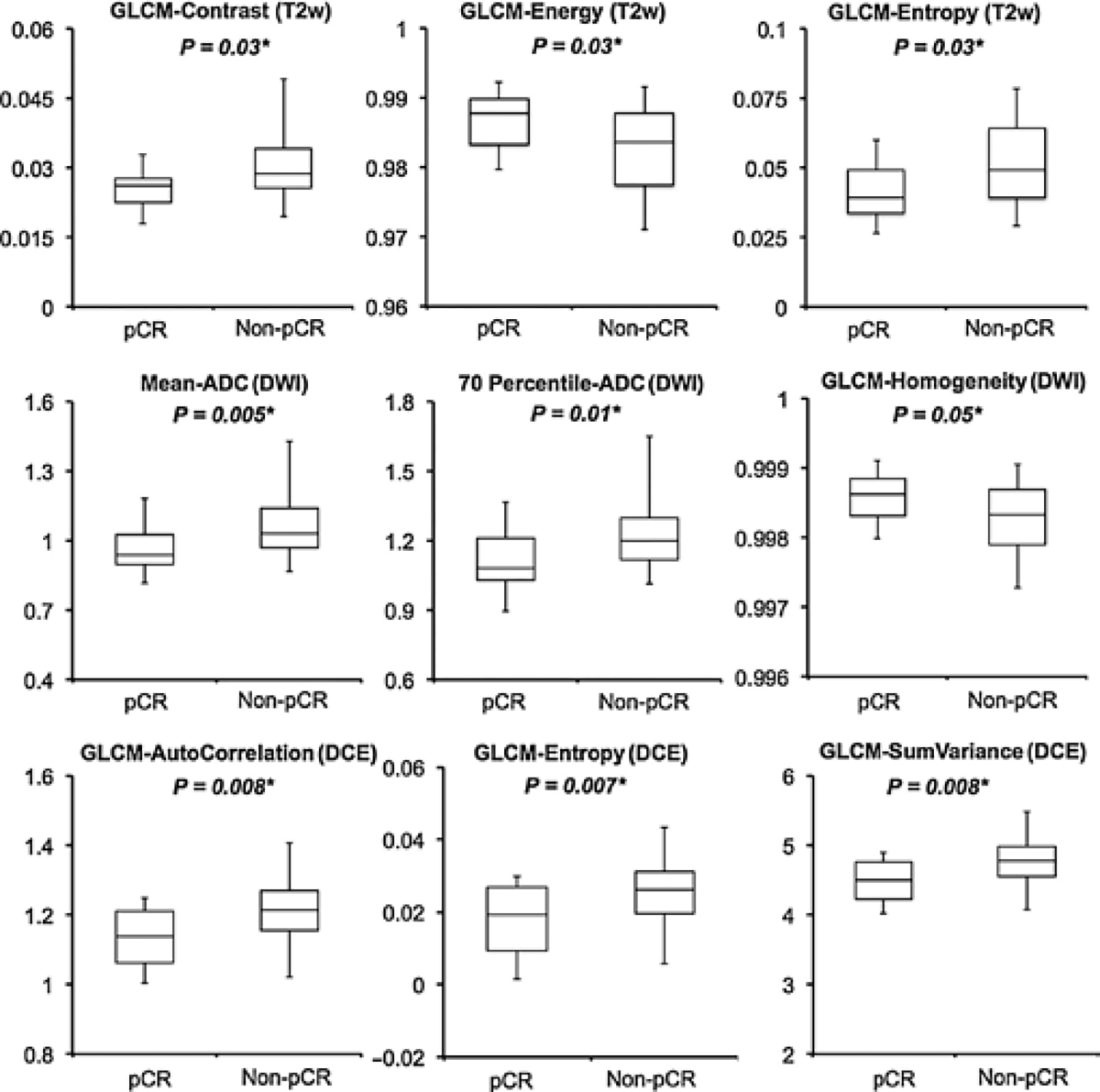
Experimental design: Forty-eight consecutive patients (January 2012-November 2014) receiving neoadjuvant CRT were enrolled. All underwent anatomical T1/T2, diffusion-weighted MRI (DWI) and dynamic contrast-enhanced (DCE) MRI before CRT. A total of 103 imaging features, analyzed using both volume-averaged and voxelized methods, were extracted for each patient. Univariate analyses were performed to evaluate the capability of each individual parameter in predicting pathologic complete response (pCR) or good response (GR) evaluated based on tumor regression grade. Artificial neural network with 4-fold validation technique was further utilized to select the best predictor sets to classify different response groups and the predictive performance was calculated using receiver operating characteristic (ROC) curves.
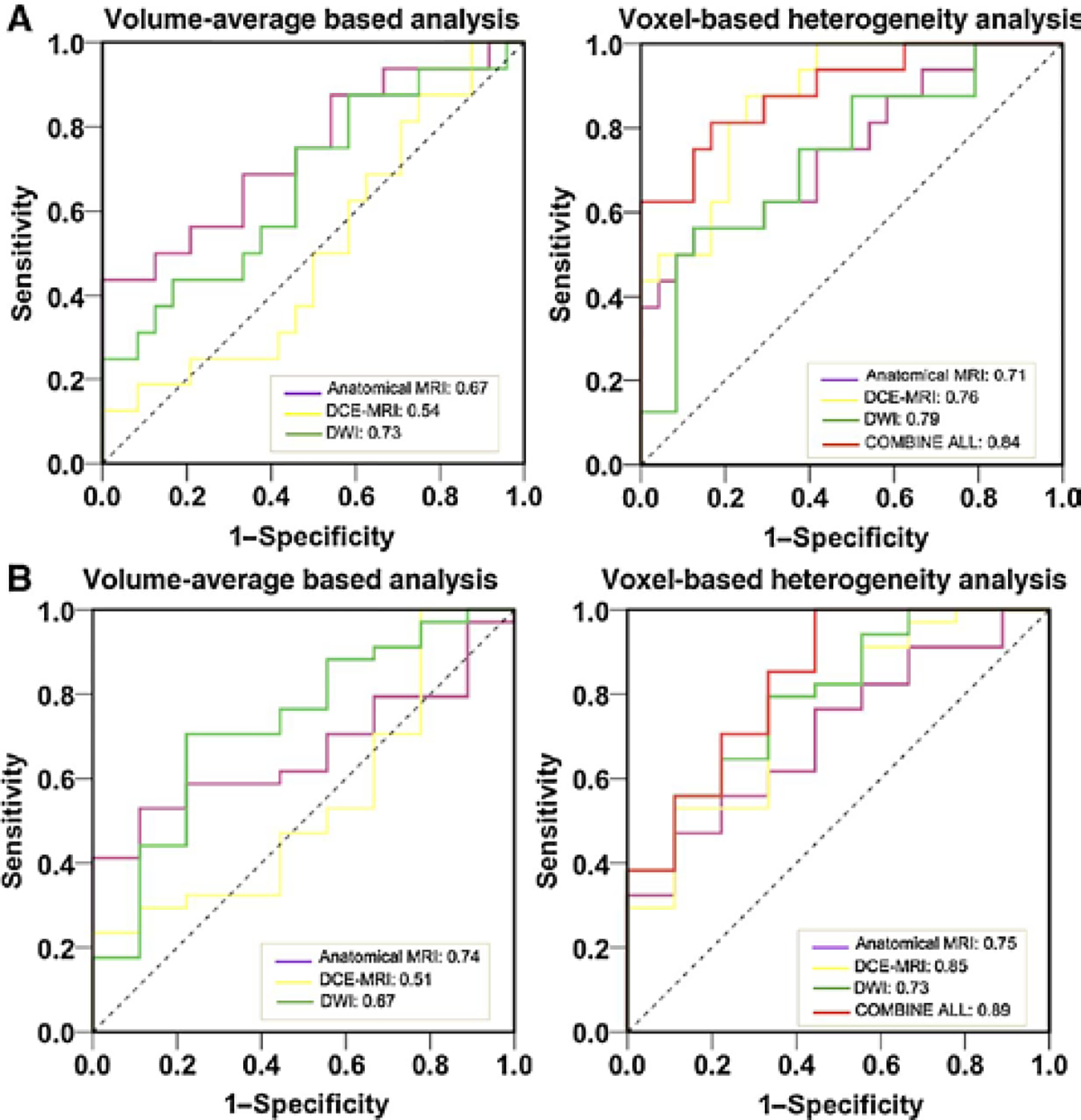
Results: The conventional volume-averaged analysis could provide an area under ROC curve (AUC) ranging from 0.54 to 0.73 in predicting pCR. While if the models were replaced by voxelized heterogeneity analysis, the prediction accuracy measured by AUC could be improved to 0.71-0.79. Similar results were found for GR prediction. In addition, each subcategory images could generate moderate power in predicting the response, which if combining all information together, the AUC could be further improved to 0.84 for pCR and 0.89 for GR prediction, respectively.
Conclusions: Through a systematic analysis of multiparametric MR imaging features, we are able to build models with improved predictive value over conventional imaging metrics. The results are encouraging, suggesting the wealth of imaging radiomics should be further explored to help tailoring the treatment into the era of personalized medicine. Clin Cancer Res; 22(21); 5256-64. ©2016 AACR.
©2016 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest
S. Jabbour reports receiving commercial research grants from Merck. No potential conflicts of interest were disclosed by the other authors.
Figures
Similar articles
-
Machine learning for prediction of chemoradiation therapy response in rectal cancer using pre-treatment and mid-radiation multi-parametric MRI.Magn Reson Imaging. 2019 Sep;61:33-40. doi: 10.1016/j.mri.2019.05.003. Epub 2019 May 3. Magn Reson Imaging. 2019. PMID: 31059768 Free PMC article.
-
Radiomics analysis of multiparametric MRI for prediction of pathological complete response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer.Eur Radiol. 2019 Mar;29(3):1211-1220. doi: 10.1007/s00330-018-5683-9. Epub 2018 Aug 20. Eur Radiol. 2019. PMID: 30128616
-
MRI radiomics combined with delta-radiomics model for predicting pathological complete response in locally advanced rectal cancer patients after neoadjuvant chemoradiotherapy: A multi-institutional study.Appl Radiat Isot. 2025 Aug;222:111842. doi: 10.1016/j.apradiso.2025.111842. Epub 2025 Apr 12. Appl Radiat Isot. 2025. PMID: 40273481
-
Machine learning in predicting pathological complete response to neoadjuvant chemoradiotherapy in rectal cancer using MRI: a systematic review and meta-analysis.Br J Radiol. 2024 Jun 18;97(1159):1243-1254. doi: 10.1093/bjr/tqae098. Br J Radiol. 2024. PMID: 38730550 Free PMC article.
-
MRI radiomics prediction modelling for pathological complete response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer: a systematic review and meta-analysis.Abdom Radiol (NY). 2025 Apr 28. doi: 10.1007/s00261-025-04953-5. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40293520 Review.
Cited by
-
Emergence of Radiomics: Novel Methodology Identifying Imaging Biomarkers of Disease in Diagnosis, Response, and Progression.SM J Clin Med Imaging. 2018;4(1):1019. Epub 2018 Mar 15. SM J Clin Med Imaging. 2018. PMID: 34109326 Free PMC article.
-
A new magnetic resonance imaging tumour response grading scheme for locally advanced rectal cancer.Br J Cancer. 2022 Jul;127(2):268-277. doi: 10.1038/s41416-022-01801-x. Epub 2022 Apr 6. Br J Cancer. 2022. PMID: 35388140 Free PMC article.
-
Pre-treatment ADC image-based random forest classifier for identifying resistant rectal adenocarcinoma to neoadjuvant chemoradiotherapy.Int J Colorectal Dis. 2020 Jan;35(1):101-107. doi: 10.1007/s00384-019-03455-3. Epub 2019 Dec 1. Int J Colorectal Dis. 2020. PMID: 31786652
-
Artificial intelligence CT radiomics to predict early recurrence of intrahepatic cholangiocarcinoma: a multicenter study.Hepatol Int. 2023 Aug;17(4):1016-1027. doi: 10.1007/s12072-023-10487-z. Epub 2023 Feb 23. Hepatol Int. 2023. PMID: 36821045
-
Predicting outcomes for locally advanced rectal cancer treated with neoadjuvant chemoradiation with CT-based radiomics.Sci Rep. 2022 Apr 13;12(1):6167. doi: 10.1038/s41598-022-10175-2. Sci Rep. 2022. PMID: 35418656 Free PMC article.
References
-
- van de Velde CJ, Boelens PG, Borras JM, Coebergh JW, Cervantes A, Blomqvist L, et al. EURECCA colorectal: multidisciplinary management: European consensus conference colon and rectum. Eur J Cancer 2014;50:1.e1–1.e34. - PubMed
-
- Kapiteijn E, Marijnen CA, Nagtegaal ID, Putter H, Steup WH, Wiggers T, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med 2001;345:638–46. - PubMed
-
- Maas M, Nelemans PJ, Valentini V, Das P, Rödel C, Kuo LJ, et al. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient data. Lancet Oncol 2010;11:835–44. - PubMed
-
- Sanghera P, Wong DW, McConkey CC, Geh JI, Hartley A. Chemoradiotherapy for rectal cancer: an updated analysis of factors affecting pathological response. Clin Oncol (R Coll Radiol) 2008;20:176–83. - PubMed
-
- Habr-Gama A, Perez RO, Proscurshim I, Campos FG, Nadalin W, Kiss D, et al. Patterns of failure and survival for nonoperative treatment of stage c0 distal rectal cancer following neoadjuvant chemoradiation therapy. J Gastrointest Surg 2006;10:1319–28. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
