

Biases in detection of apparent "weekend effect" on outcome with administrative coding data: population based study of stroke
- PMID: 27185754
- PMCID: PMC4868367
- DOI: 10.1136/bmj.i2648
Biases in detection of apparent "weekend effect" on outcome with administrative coding data: population based study of stroke
Abstract
Objectives: To determine the accuracy of coding of admissions for stroke on weekdays versus weekends and any impact on apparent outcome.
Design: Prospective population based stroke incidence study and a scoping review of previous studies of weekend effects in stroke.
Setting: Primary and secondary care of all individuals registered with nine general practices in Oxfordshire, United Kingdom (OXVASC, the Oxford Vascular Study).
Participants: All patients with clinically confirmed acute stroke in OXVASC identified with multiple overlapping methods of ascertainment in 2002-14 versus all acute stroke admissions identified by hospital diagnostic and mortality coding alone during the same period.
Main outcomes measures: Accuracy of administrative coding data for all patients with confirmed stroke admitted to hospital in OXVASC. Difference between rates of "false positive" or "false negative" coding for weekday and weekend admissions. Impact of inaccurate coding on apparent case fatality at 30 days in weekday versus weekend admissions. Weekend effects on outcomes in patients with confirmed stroke admitted to hospital in OXVASC and impacts of other potential biases compared with those in the scoping review.
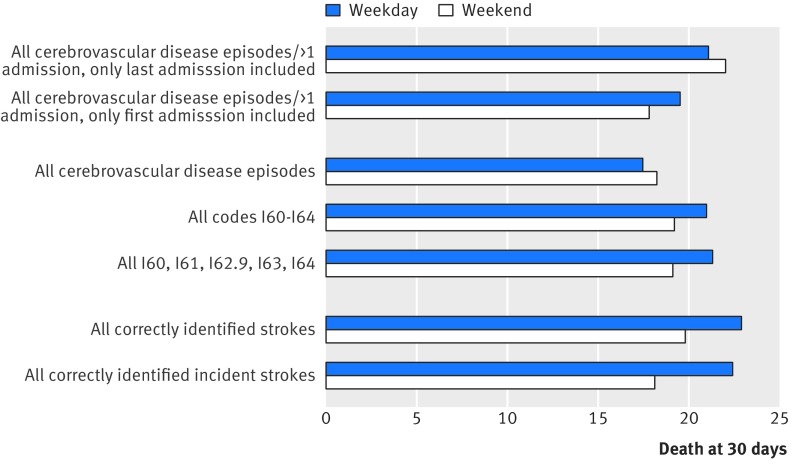
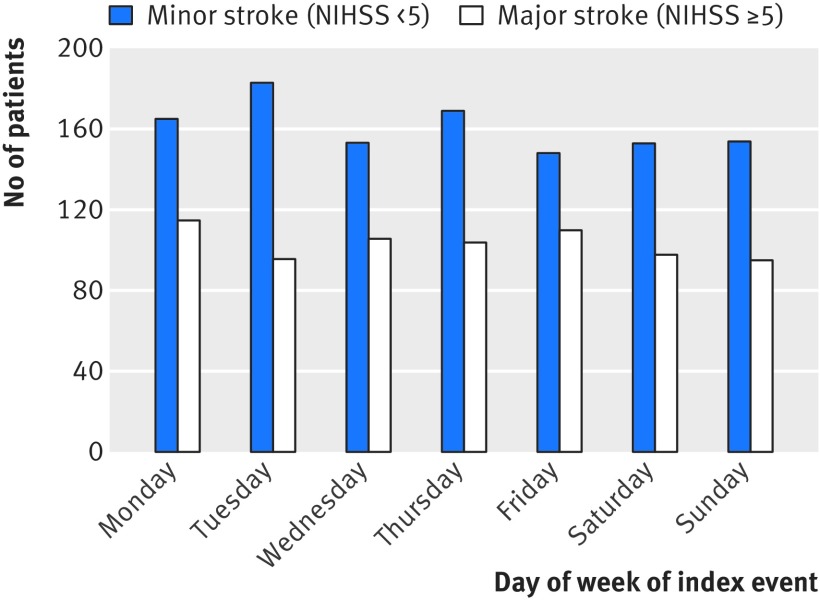
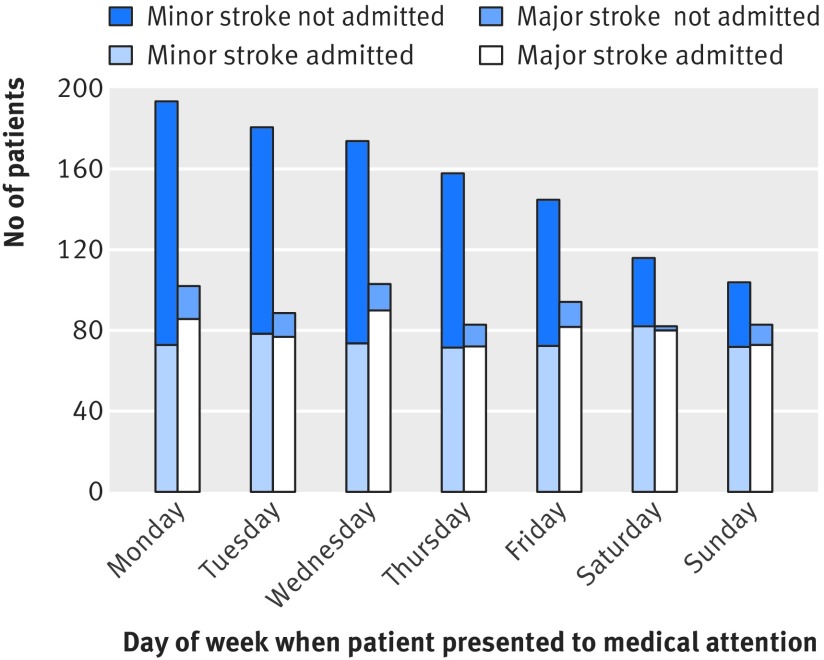
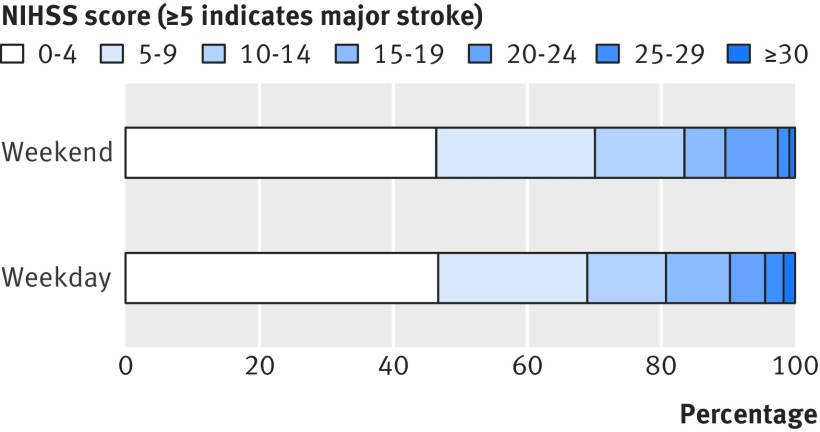
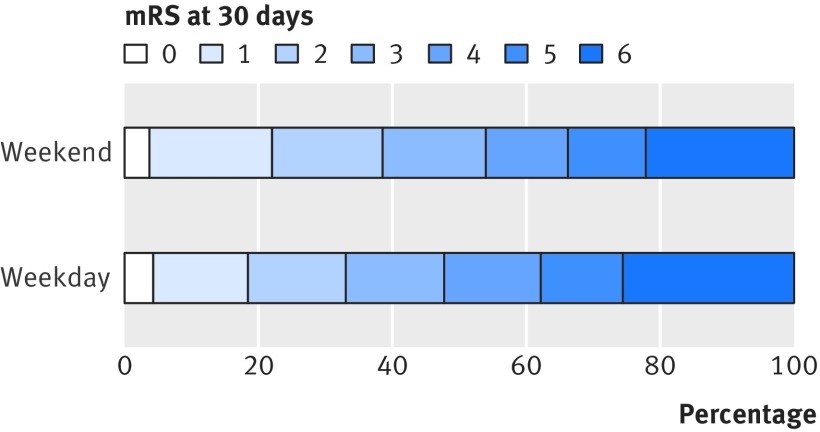
Results: Among 92 728 study population, 2373 episodes of acute stroke were ascertained in OXVASC, of which 826 (34.8%) mainly minor events were managed without hospital admission, 60 (2.5%) occurred out of the area or abroad, and 195 (8.2%) occurred in hospital during an admission for a different reason. Of 1292 local hospital admissions for acute stroke, 973 (75.3%) were correctly identified by administrative coding. There was no bias in distribution of weekend versus weekday admission of the 319 strokes missed by coding. Of 1693 admissions for stroke identified by coding, 1055 (62.3%) were confirmed to be acute strokes after case adjudication. Among the 638 false positive coded cases, patients were more likely to be admitted on weekdays than at weekends (536 (41.0%) v 102 (26.5%); P<0.001), partly because of weekday elective admissions after previous stroke being miscoded as new stroke episodes (267 (49.8%) v 26 (25.5%); P<0.001). The 30 day case fatality after these elective admissions was lower than after confirmed acute stroke admissions (11 (3.8%) v 233 (22.1%); P<0.001). Consequently, relative 30 day case fatality for weekend versus weekday admissions differed (P<0.001) between correctly coded acute stroke admissions and false positive coding cases. Results were consistent when only the 1327 emergency cases identified by "admission method" from coding were included, with more false positive cases with low case fatality (35 (14.7%)) being included for weekday versus weekend admissions (190 (19.5%) v 48 (13.7%), P<0.02). Among all acute stroke admissions in OXVASC, there was no imbalance in baseline stroke severity for weekends versus weekdays and no difference in case fatality at 30 days (adjusted odds ratio 0.85, 95% confidence interval 0.63 to 1.15; P=0.30) or any adverse "weekend effect" on modified Rankin score at 30 days (0.78, 0.61 to 0.99; P=0.04) or one year (0.76, 0.59 to 0.98; P=0.03) among incident strokes.
Conclusion: Retrospective studies of UK administrative hospital coding data to determine "weekend effects" on outcome in acute medical conditions, such as stroke, can be undermined by inaccurate coding, which can introduce biases that cannot be reliably dealt with by adjustment for case mix.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Pitfalls of administrative database analysis are evident when assessing the 'weekend effect' in stroke.Evid Based Med. 2017 Mar;22(1):35. doi: 10.1136/ebmed-2016-110557. Epub 2016 Nov 4. Evid Based Med. 2017. PMID: 27815303 No abstract available.
References
-
- Bell CM, Redelmeier DA. Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med 2001;345:663-8. 10.1056/NEJMsa003376 pmid:11547721. - DOI - PubMed
-
- Freemantle N, Richardson M, Wood J, et al. Weekend hospitalization and additional risk of death: an analysis of inpatient data. J R Soc Med 2012;105:74-84. 10.1258/jrsm.2012.120009 pmid:22307037. - DOI - PMC - PubMed
-
- Freemantle N, Ray D, McNulty D, et al. Increased mortality associated with weekend hospital admission: a case for expanded seven day services?BMJ 2015;351:h4596 10.1136/bmj.h4596. pmid:26342923. - DOI - PubMed
-
- Concha OP, Gallego B, Hillman K, Delaney GP, Coiera E. Do variations in hospital mortality patterns after weekend admission reflect reduced quality of care or different patient cohorts? A population-based study. BMJ Qual Saf 2014;23:215-22. 10.1136/bmjqs-2013-002218 pmid:24163392. - DOI - PMC - PubMed
-
- Vest-Hansen B, Riis AH, Sørensen HT, Christiansen CF. Out-of-hours and weekend admissions to Danish medical departments: admission rates and 30-day mortality for 20 common medical conditions. BMJ Open 2015;5:e006731 10.1136/bmjopen-2014-006731. pmid:25762233. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical