

Minimal Treatment of Low-Risk, Pediatric Lymphocyte-Predominant Hodgkin Lymphoma: A Report From the Children's Oncology Group
- PMID: 27185849
- PMCID: PMC4981978
- DOI: 10.1200/JCO.2015.65.3469
Minimal Treatment of Low-Risk, Pediatric Lymphocyte-Predominant Hodgkin Lymphoma: A Report From the Children's Oncology Group
Abstract
Purpose: Children's Oncology Group study AHOD03P1 was designed to determine whether excellent outcomes can be maintained for patients with low-risk, pediatric lymphocyte-predominant Hodgkin lymphoma (LPHL) with a strategy of resection alone or minimal chemotherapy.
Patients and methods: Patients with stage IA LPHL in a single node that was completely resected were observed without further therapy; recurrences were treated with three cycles of doxorubicin/vincristine/prednisone/cyclophosphamide (AV-PC). Patients with unresected stage IA or stage IIA LPHL were treated with three cycles of AV-PC. Patients with less than a complete response (CR) to AV-PC received 21-Gy involved-field radiation therapy (IFRT).
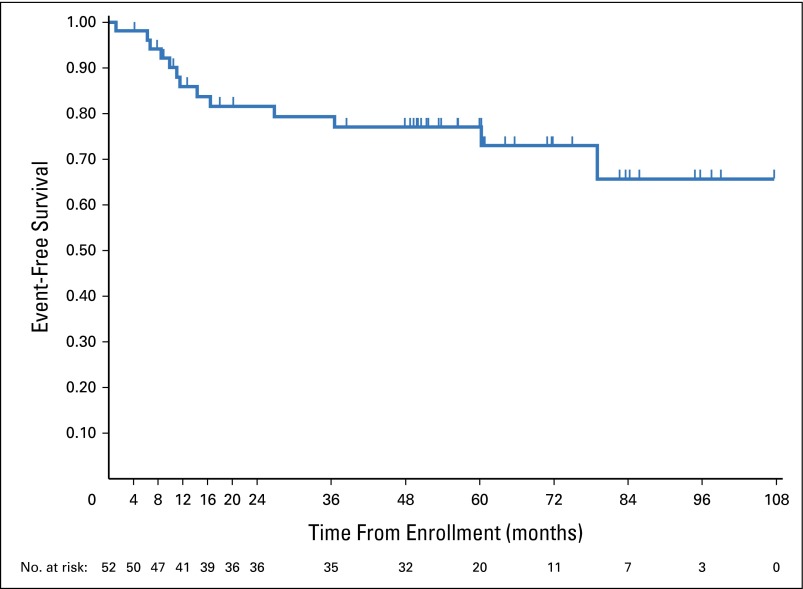
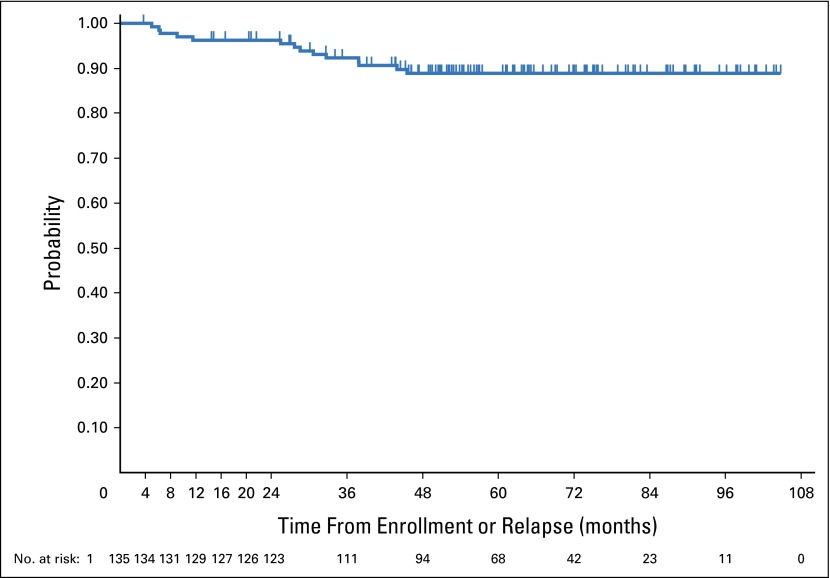
Results: A total of 183 eligible patients were enrolled; 178 were evaluable. Of these, 52 patients underwent complete resection of a single node. There were 13 relapses at a median of 11.5 months; 5-year event-free survival (EFS) was 77% (range, 62% to 87%). A total of 135 patients received AV-PC; 126 were treated at diagnosis and nine at relapse after surgery alone. Eleven patients receiving AV-PC had less than CR and received IFRT. Fourteen first events occurred among 135 patients (12 relapses and two second malignancies). Two relapses occurred in patients who had received IFRT. Five-year EFS was 88.8% (95% CI, 81.8% to 93.2%). Five-year EFS for the entire cohort was 85.5% (95% CI, 79.2% to 90.1%); overall survival was 100%.
Conclusion: Some 75% of highly selected pediatric patients with LPHL may be spared chemotherapy after surgical resection alone. Pediatric LPHL has excellent EFS with chemotherapy that is less intensive than standard regimens; > 90% of patients can avoid radiation therapy. The salvage rate for the few relapses is high, with 100% survival overall.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- Marafioti T, Hummel M, Anagnostopoulos I, et al. Origin of nodular lymphocyte-predominant Hodgkin’s disease from a clonal expansion of highly mutated germinal-center B cells. N Engl J Med. 1997;337:453–458. - PubMed
-
- Ohno T, Stribley JA, Wu G, et al. Clonality in nodular lymphocyte-predominant Hodgkin’s disease. N Engl J Med. 1997;337:459–466. - PubMed
-
- Harris NL. Shades of gray between large B-cell lymphomas and Hodgkin lymphomas: Differential diagnosis and biological implications. Mod Pathol. 2013;26:S57–S70. (suppl 1) - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
