

The pathophysiology of thrombocytopenia in chronic liver disease
- PMID: 27186144
- PMCID: PMC4847598
- DOI: 10.2147/HMER.S74612
The pathophysiology of thrombocytopenia in chronic liver disease
Abstract
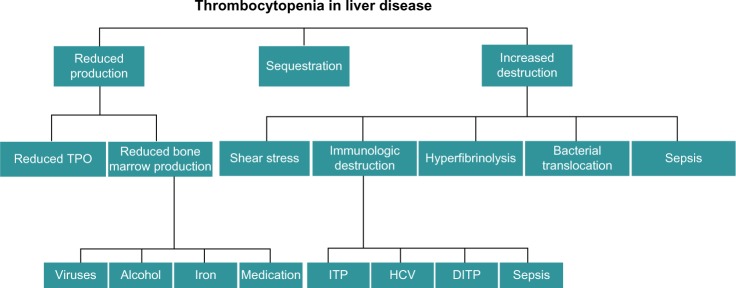
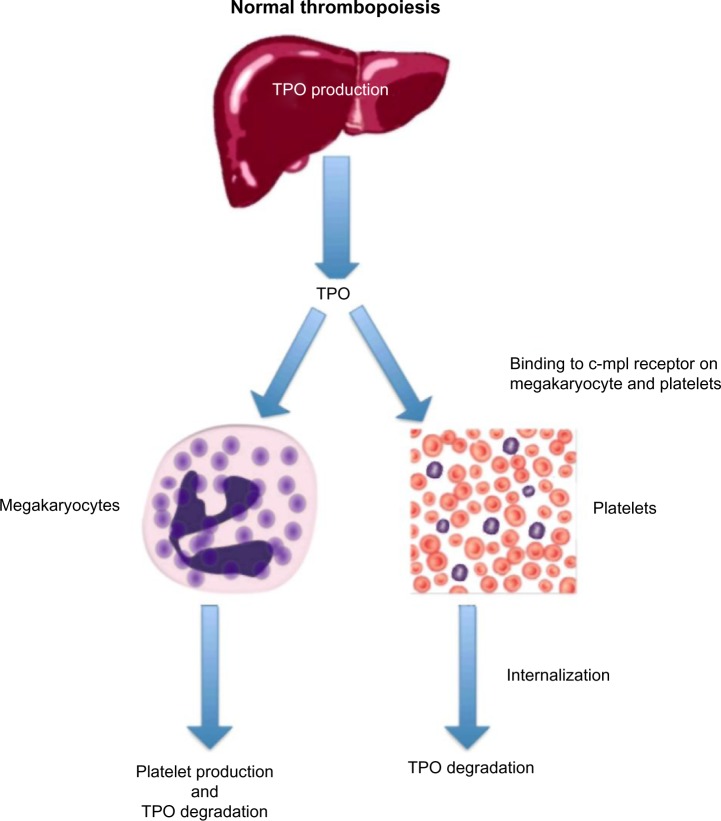
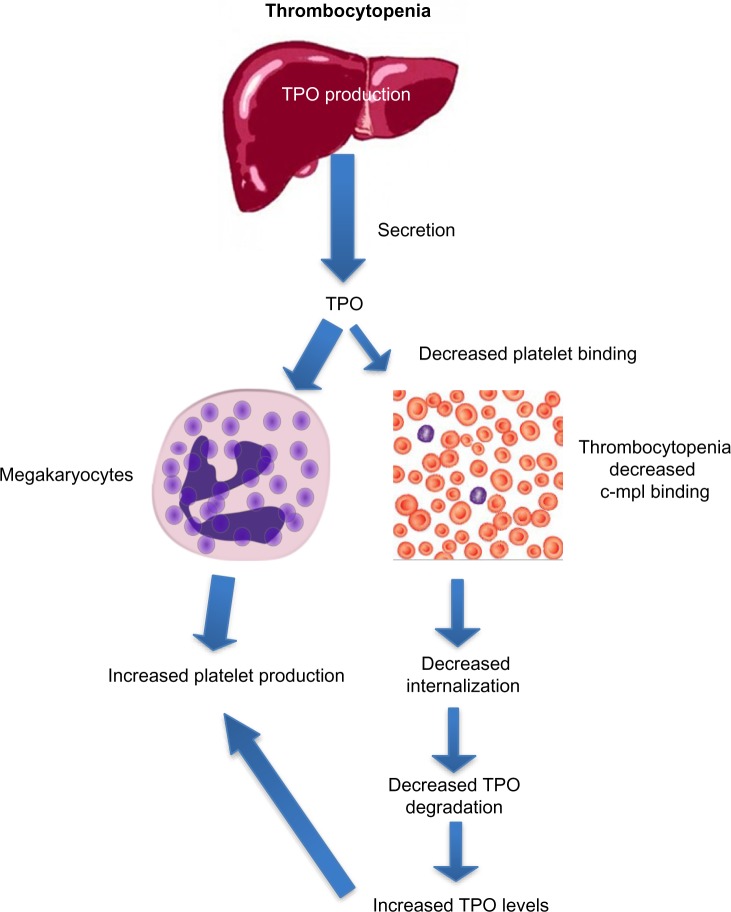
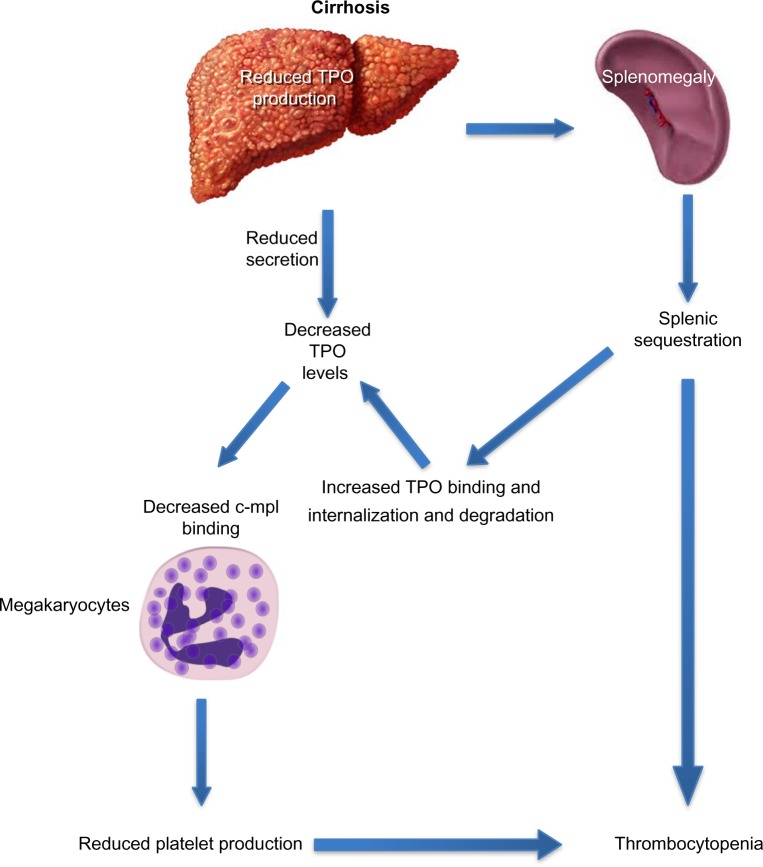
Thrombocytopenia is the most common hematological abnormality encountered in patients with chronic liver disease (CLD). In addition to being an indicator of advanced disease and poor prognosis, it frequently prevents crucial interventions. Historically, thrombocytopenia has been attributed to hypersplenism, which is the increased pooling of platelets in a spleen enlarged by congestive splenomegaly secondary to portal hypertension. Over the past decade, however, there have been significant advances in the understanding of thrombopoiesis, which, in turn, has led to an improved understanding of thrombocytopenia in cirrhosis. Multiple factors contribute to the development of thrombocytopenia and these can broadly be divided into those that cause decreased production, splenic sequestration, and increased destruction. Depressed thrombopoietin levels in CLD, together with direct bone marrow suppression, result in a reduced rate of platelet production. Thrombopoietin regulates both platelet production and maturation and is impaired in CLD. Bone marrow suppression can be caused by viruses, alcohol, iron overload, and medications. Splenic sequestration results from hypersplenism. The increased rate of platelet destruction in cirrhosis also occurs through a number of pathways: increased shear stress, increased fibrinolysis, bacterial translocation, and infection result in an increased rate of platelet aggregation, while autoimmune disease and raised titers of antiplatelet immunoglobulin result in the immunologic destruction of platelets. An in-depth understanding of the complex pathophysiology of the thrombocytopenia of CLD is crucial when considering treatment strategies. This review outlines the recent advances in our understanding of thrombocytopenia in cirrhosis and CLD.
Keywords: cirrhosis; thrombocytopenia; thrombopoietin.
Figures
References
-
- Bashour FN, Teran JC, Mullen KD. Prevalence of peripheral blood cytopenias (hypersplenism) in patients with nonalcoholic chronic liver disease. Am J Gastroenterol. 2000;95(10):2936–2939. - PubMed
-
- Poynard T, Bedossa P. Age and platelet count: a simple index for predicting the presence of histological lesions in patients with antibodies to hepatitis C virus. METAVIR and CLINIVIR Cooperative Study Groups. J Viral Hepat. 1997;4(3):199–208. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
