

Case Reports
doi: 10.2484/rcr.v9i3.971.
eCollection 2014.
Tuberculous peritonitis
- PMID: 27186257
- PMCID: PMC4861862
- DOI: 10.2484/rcr.v9i3.971
Item in Clipboard
Case Reports
Tuberculous peritonitis
Radiol Case Rep.
.
Abstract
Tuberculous peritonitis is a serious condition with rising prevalence in recent years. It is especially common in those patients with risk factors such as an immunocompromised state, chronic kidney disease, or cirrhosis/liver disease. Spread is typically hematogenous from pulmonary foci. We report on a 34-year-old man who presented with initial complaints of cough, low-grade fevers, abdominal pain, and nausea/vomiting. Chest x-ray showed a cluster of nodular opacities on the right upper lobe, and a CT scan showed diffuse thickening and nodularity of the omentum with prominent mesenteric lymph nodes, consistent with tuberculous peritonitis.
Figures
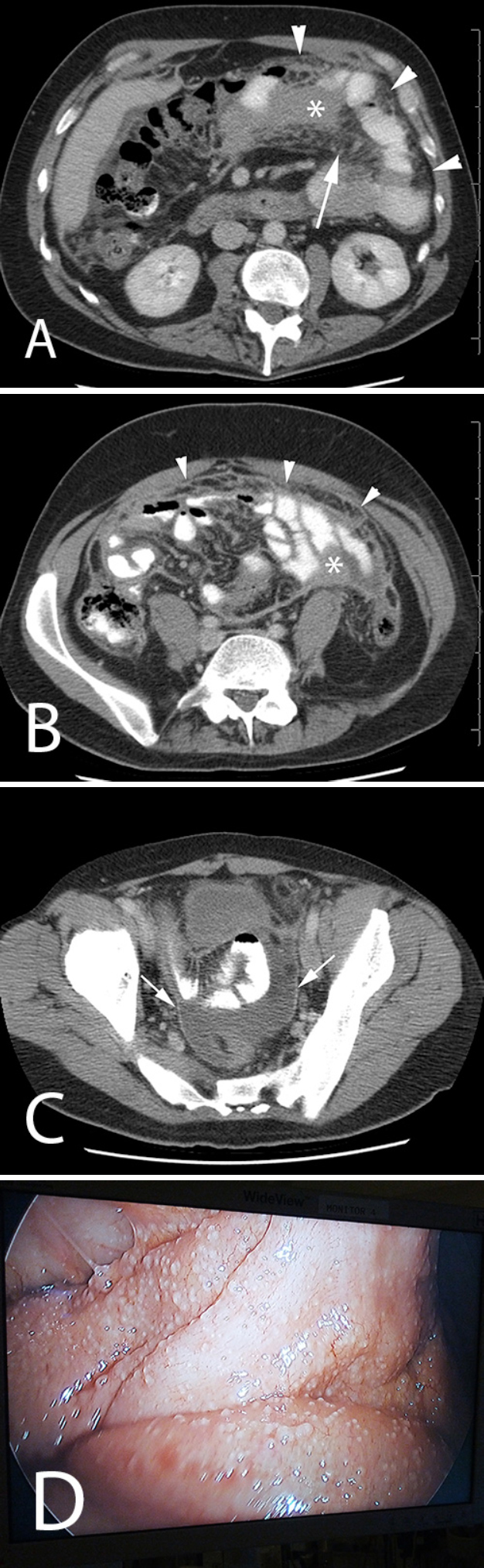
Postcontrast CT at the level of the kidneys shows diffuse thickening and nodularity of the omentum (arrowheads in A, B), infiltration of the mesentery (arrow), and a small amount of hemoperitoneum (asterisks in A, B). In B, more inferiorly, note multiple prominent mesenteric lymph nodes and diffuse thickening of the small bowel. In C, in the pelvis, note a small volume of ascites in the rectovesicle space and enhancement of the peritoneal reflections due to peritonitis. D, a photograph taken during laparoscopic biopsy, that shows the innumerable micronodules covering the surface of the small bowel. Histologically, these micronodules were found to have caseating and noncaseating granulomatous inflammation with acidfast organisms, consistent with tuberculosis.
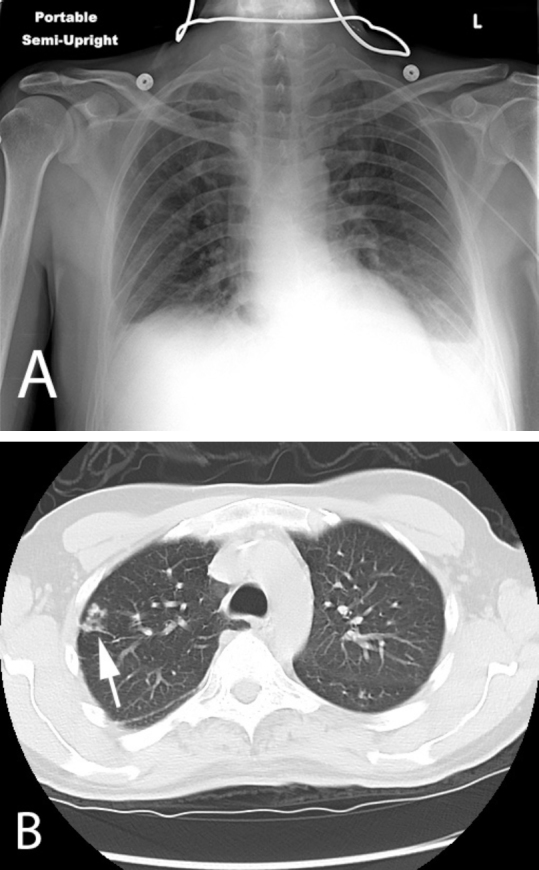
A) Portable chest radiograph and B) CT showing a subtle cluster of airspace opacities in the right upper lobe (arrow).
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
