

Association of Acute Gastroesophageal Reflux Disease With Esophageal Histologic Changes
- PMID: 27187303
- PMCID: PMC5030713
- DOI: 10.1001/jama.2016.5657
Association of Acute Gastroesophageal Reflux Disease With Esophageal Histologic Changes
Abstract
Importance: The histologic changes associated with acute gastroesophageal reflux disease (GERD) have not been studied prospectively in humans. Recent studies in animals have challenged the traditional notion that reflux esophagitis develops when esophageal surface epithelial cells are exposed to lethal chemical injury from refluxed acid.
Objective: To evaluate histologic features of esophageal inflammation in acute GERD to study its pathogenesis.
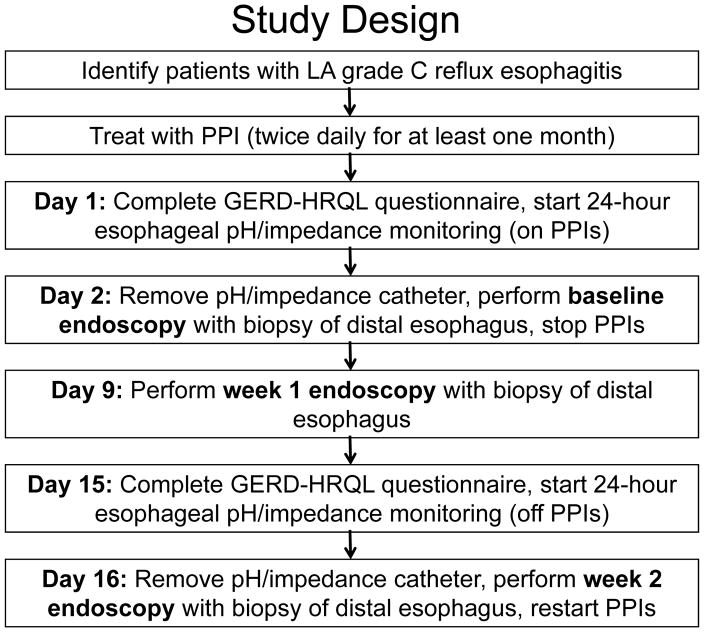
Design, setting, and participants: Patients from the Dallas Veterans Affairs Medical Center who had reflux esophagitis successfully treated with proton pump inhibitors (PPIs) began 24-hour esophageal pH and impedance monitoring and esophagoscopy (including confocal laser endomicroscopy [CLE]) with biopsies from noneroded areas of distal esophagus at baseline (taking PPIs) and at 1 week and 2 weeks after stopping the PPI medication. Enrollment began May 2013 and follow-up ended July 2015.
Interventions: PPIs stopped for 2 weeks.
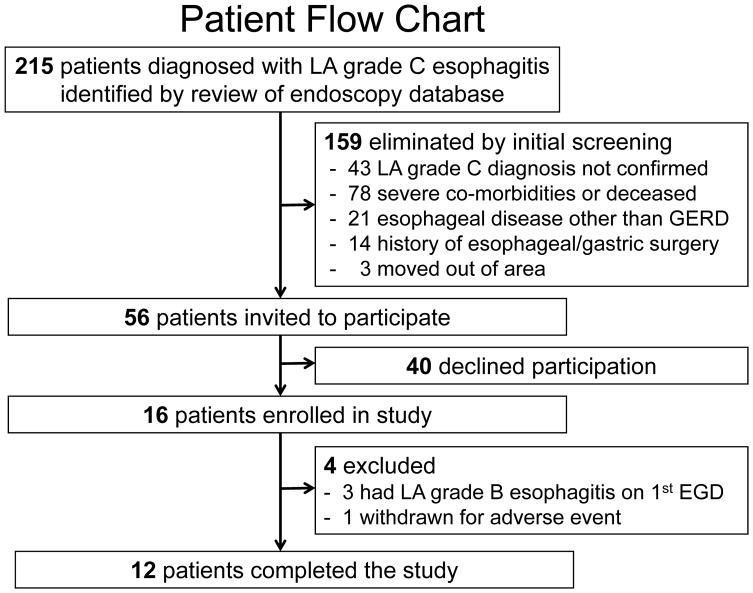
Main outcomes and measures: Twelve patients (men, 11; mean age, 57.6 year [SD, 13.1]) completed the study. Primary outcome was change in esophageal inflammation 2 weeks after stopping the PPI medication, determined by comparing lymphocyte, eosinophil, and neutrophil infiltrates (each scored on a 0-3 scale) in esophageal biopsies. Also evaluated were changes in epithelial basal cell and papillary hyperplasia, surface erosions, intercellular space width, endoscopic grade of esophagitis, esophageal acid exposure, and mucosal impedance (an index of mucosal integrity).
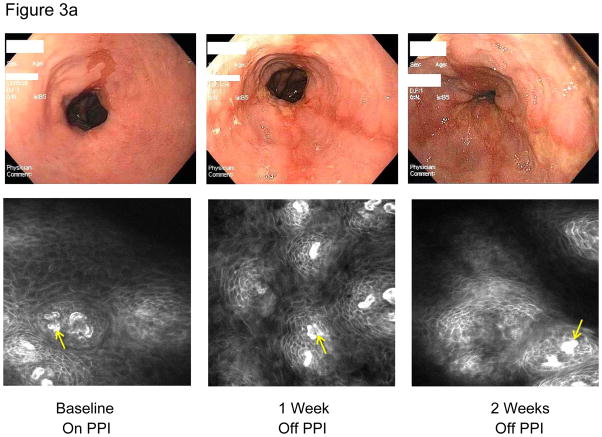
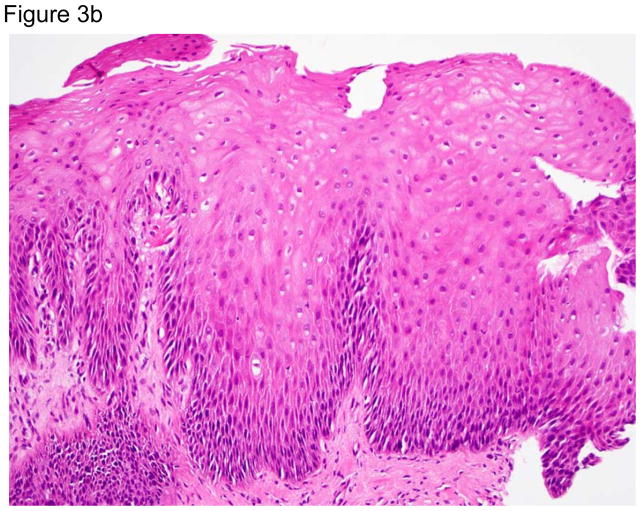
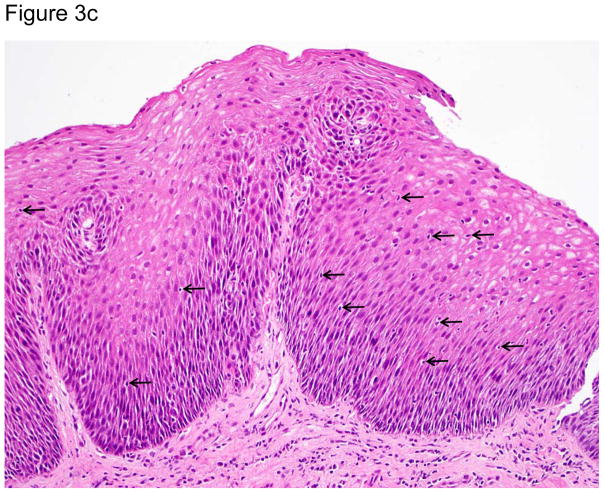
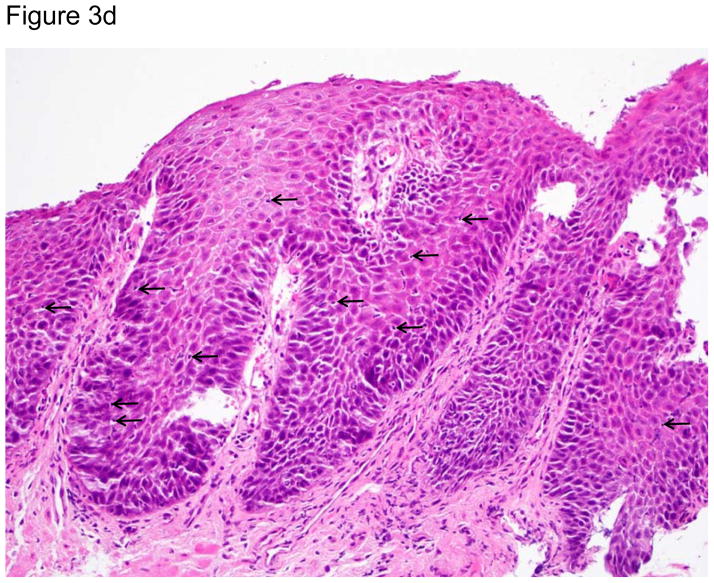
Results: At 1 week and 2 weeks after discontinuation of PPIs, biopsies showed significant increases in intraepithelial lymphocytes, which were predominantly T cells (median [range]: 0 (0-2) at baseline vs 1 (1-2) at both 1 week [P = .005] and 2 weeks [P = .002]); neutrophils and eosinophils were few or absent. Biopsies also showed widening of intercellular spaces (confirmed by CLE), and basal cell and papillary hyperplasia developed without surface erosions. Two weeks after stopping the PPI medication, esophageal acid exposure increased (median: 1.2% at baseline to 17.8% at 2 weeks; Δ, 16.2% [95% CI, 4.4%-26.5%], P = .005), mucosal impedance decreased (mean: 2671.3 Ω at baseline to 1508.4 Ω at 2 weeks; Δ, 1162.9 Ω [95% CI, 629.9-1695.9], P = .001), and all patients had evidence of esophagitis.
Conclusions and relevance: In this preliminary study of 12 patients with severe reflux esophagitis successfully treated with PPI therapy, stopping PPI medication was associated with T lymphocyte-predominant esophageal inflammation and basal cell and papillary hyperplasia without loss of surface cells. If replicated, these findings suggest that the pathogenesis of reflux esophagitis may be cytokine-mediated rather than the result of chemical injury.
Trial registration: clinicaltrials.gov Identifier: NCT01733810.
Figures
Comment in
-
Turning the Pathogenesis of Acute Peptic Esophagitis Inside Out.JAMA. 2016 May 17;315(19):2077-8. doi: 10.1001/jama.2016.5827. JAMA. 2016. PMID: 27187299 No abstract available.
-
GERD: A challenge to our view of reflux oesophagitis pathogenesis.Nat Rev Gastroenterol Hepatol. 2016 Sep;13(9):504-5. doi: 10.1038/nrgastro.2016.106. Epub 2016 Jul 13. Nat Rev Gastroenterol Hepatol. 2016. PMID: 27407046 No abstract available.
References
-
- Locke GR, 3rd, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ., 3rd Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112(5):1448–56. - PubMed
-
- Winkelstein A. Peptic esophagitis: a new clinical entity. JAMA. 1935;104(11):906–9.
-
- Ismail-Beigi F, Horton PF, Pope CE., 2nd Histological consequences of gastroesophageal reflux in man. Gastroenterology. 1970;58(2):163–74. - PubMed
-
- Fiocca R, Mastracci L, Riddell R, Takubo K, Vieth M, Yerian L, Sharma P, Fernström P, Ruth M. Development of consensus guidelines for the histologic recognition of microscopic esophagitis in patients with gastroesophageal reflux disease: the Esohisto project. Hum Pathol. 2010;41(2):223–31. - PubMed
-
- Eastwood GL. Histologic changes in gastroesophageal reflux. J Clin Gastroenterol. 1986;8(Suppl 1):45–51. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
