

Comparative Safety of Pharmacologic Treatments for Persistent Depressive Disorder: A Systematic Review and Network Meta-Analysis
- PMID: 27187783
- PMCID: PMC4871495
- DOI: 10.1371/journal.pone.0153380
Comparative Safety of Pharmacologic Treatments for Persistent Depressive Disorder: A Systematic Review and Network Meta-Analysis
Abstract
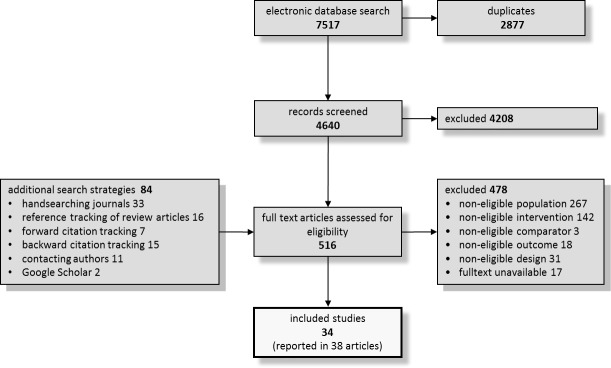
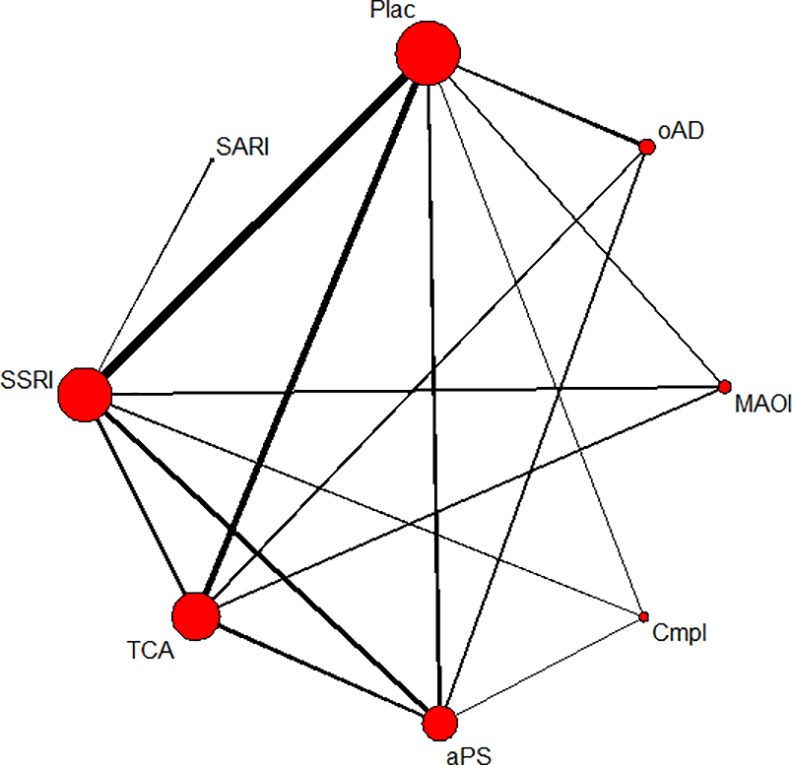
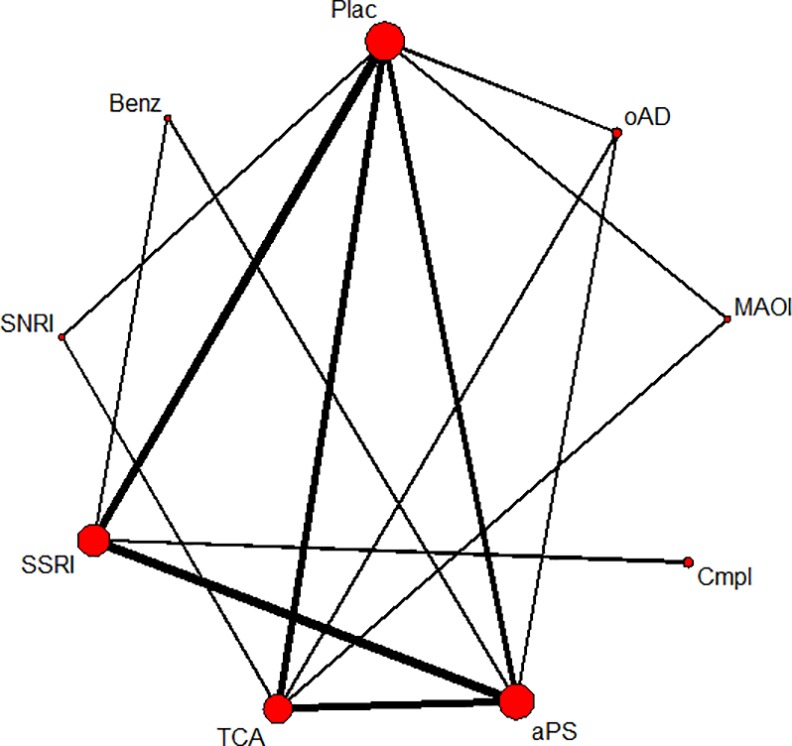
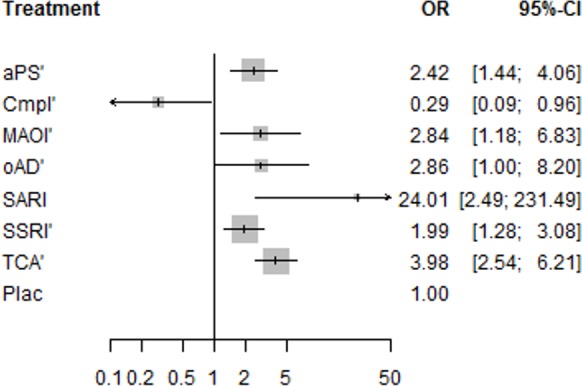
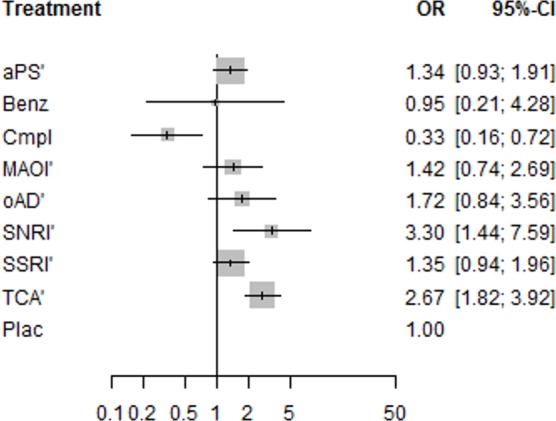
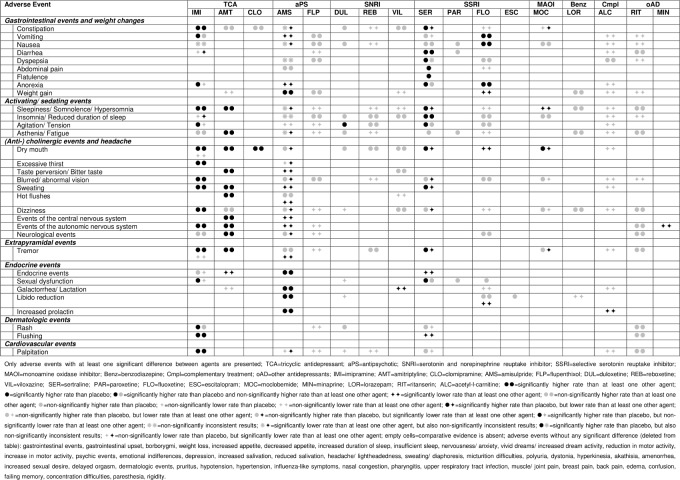
We aimed to compare the safety of antidepressants for the treatment of persistent depressive disorder (PDD) with each other and with placebo. We conducted a systematic electronic search and included randomized controlled trials that investigated antidepressants for the treatment of PDD in adults. Outcomes were the incidence of experiencing any adverse event, specific adverse events and related treatment discontinuations. We analyzed the data using traditional and network meta-analyses. Thirty-four studies that comprised 4,769 patients and examined 20 individual agents in nine substance classes were included. Almost all analyzed substance classes were associated with higher discontinuation rates than placebo including tricyclic antidepressants (TCAs), selective serotonin reuptake inhibitors (SSRIs), monoamine oxidase inhibitors (MAOIs), antipsychotics, and the serotonin antagonist and reuptake inhibitor (SARI) trazodone. The odds of experiencing any adverse event were significantly higher for TCAs and serotonin noradrenaline reuptake inhibitors (SNRIs) compared to placebo. Pairwise comparisons among the substance classes revealed that more patients receiving TCAs or SNRIs experienced any adverse event and that more patients receiving TCAs or the SARI trazodone discontinued treatment. The complementary treatment with acetyl-l-carnitine showed lower rates of experiencing any adverse event and related discontinuations than all other comparators. TCAs were primarily associated with (anti-)cholinergic and sedating adverse events. SSRIs primarily showed gastrointestinal adverse events. Patients treated with the antipsychotic amisulpride were more likely to manifest weight gain and endocrine adverse events. The comparative evidence for further agents was insufficient or lacking. The identified safety differences may be used to inform the selection among the antidepressants.
Conflict of interest statement
Figures
Similar articles
-
Pharmacological treatments in panic disorder in adults: a network meta-analysis.Cochrane Database Syst Rev. 2023 Nov 28;11(11):CD012729. doi: 10.1002/14651858.CD012729.pub3. Cochrane Database Syst Rev. 2023. PMID: 38014714 Free PMC article.
-
Antidepressants versus placebo for panic disorder in adults.Cochrane Database Syst Rev. 2018 Apr 5;4(4):CD010676. doi: 10.1002/14651858.CD010676.pub2. Cochrane Database Syst Rev. 2018. PMID: 29620793 Free PMC article.
-
Vortioxetine for depression in adults.Cochrane Database Syst Rev. 2017 Jul 5;7(7):CD011520. doi: 10.1002/14651858.CD011520.pub2. Cochrane Database Syst Rev. 2017. PMID: 28677828 Free PMC article.
-
New generation antidepressants for depression in children and adolescents: a network meta-analysis.Cochrane Database Syst Rev. 2021 May 24;5(5):CD013674. doi: 10.1002/14651858.CD013674.pub2. Cochrane Database Syst Rev. 2021. PMID: 34029378 Free PMC article.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
Cited by
-
Characteristics of persistent depression in the long-term: Randomized controlled trial and two-year observational study.Heliyon. 2023 Oct 13;9(10):e20917. doi: 10.1016/j.heliyon.2023.e20917. eCollection 2023 Oct. Heliyon. 2023. PMID: 37886758 Free PMC article.
-
Carnitine and Depression.Front Nutr. 2022 Mar 14;9:853058. doi: 10.3389/fnut.2022.853058. eCollection 2022. Front Nutr. 2022. PMID: 35369081 Free PMC article. Review.
-
Amantadine in Treatment of Dysthymia-The Pilot Case Series Study.Pharmaceuticals (Basel). 2023 Jun 19;16(6):897. doi: 10.3390/ph16060897. Pharmaceuticals (Basel). 2023. PMID: 37375844 Free PMC article.
-
Efficacy and tolerability of fluvoxamine in adults with social anxiety disorder: A meta-analysis.Medicine (Baltimore). 2018 Jul;97(28):e11547. doi: 10.1097/MD.0000000000011547. Medicine (Baltimore). 2018. PMID: 29995828 Free PMC article. Review.
-
Dynamic Changes in Plasma Metabolic Profiles Reveal a Potential Metabolite Panel for Interpretation of Fatal Intoxication by Chlorpromazine or Olanzapine in Mice.Metabolites. 2022 Nov 27;12(12):1184. doi: 10.3390/metabo12121184. Metabolites. 2022. PMID: 36557223 Free PMC article.
References
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62: 593–602. - PubMed
-
- Klein DN. Chronic depression: diagnosis and classification. Curr Dir Psychol Sci. 2010;19: 96–100.
-
- Torpey DC, Klein DN. Chronic depression: update on classification and treatment. Curr Psychiatry Rep. 2008;10: 458–464. - PubMed
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, fifth ed. (DSM 5). Arlington: American Psychiatric Publishing; 2013.
-
- De Lima MS, Moncrieff J, Soares B. Drugs versus placebo for dysthymia. Cochrane Database Syst Rev. 2005;2:CD001130. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
