

Erectile dysfunction
- PMID: 27188339
- PMCID: PMC5027992
- DOI: 10.1038/nrdp.2016.3
Erectile dysfunction
Abstract
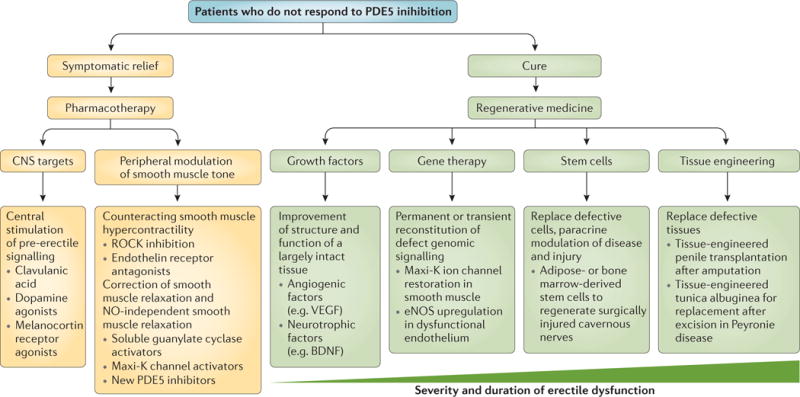
Erectile dysfunction is a multidimensional but common male sexual dysfunction that involves an alteration in any of the components of the erectile response, including organic, relational and psychological. Roles for nonendocrine (neurogenic, vasculogenic and iatrogenic) and endocrine pathways have been proposed. Owing to its strong association with metabolic syndrome and cardiovascular disease, cardiac assessment may be warranted in men with symptoms of erectile dysfunction. Minimally invasive interventions to relieve the symptoms of erectile dysfunction include lifestyle modifications, oral drugs, injected vasodilator agents and vacuum erection devices. Surgical therapies are reserved for the subset of patients who have contraindications to these nonsurgical interventions, those who experience adverse effects from (or are refractory to) medical therapy and those who also have penile fibrosis or penile vascular insufficiency. Erectile dysfunction can have deleterious effects on a man's quality of life; most patients have symptoms of depression and anxiety related to sexual performance. These symptoms, in turn, affect his partner's sexual experience and the couple's quality of life. This Primer highlights numerous aspects of erectile dysfunction, summarizes new treatment targets and ongoing preclinical studies that evaluate new pharmacotherapies, and covers the topic of regenerative medicine, which represents the future of sexual medicine.
Conflict of interest statement
The other authors declare no competing interests.
Figures
References
-
- Virag R, Zwang G, Dermange H, Legman M. Vasculogenic impotence: a review of 92 cases with 54 surgical operations. Vasc Surg. 1981;15:9–17.
-
- Glina S, Shindel A, Eardley I, Ghanem H. Cavernosal α-blockade: a new technique for investigating and treating erectile impotence by GS Brindley. J Sex Med. 2008;5:1791–1794. - PubMed
-
- Scott FB, Bradley WE, Timm GW. Management of erectile impotence. Use of implantable inflatable prosthesis. Urology. 1973;2:80–82. - PubMed
-
- Blumenthal SA. Earl Sutherland (1915–1974) [corrected] and the discovery of cyclic AMP. Perspect Biol Med. 2012;55:236–249. - PubMed
-
- Ballard SA, et al. Effects of sildenafil on the relaxation of human corpus cavernosum tissue in vitro and on the activities of cyclic nucleotide phosphodiesterase isozymes. J Urol. 1998;159:2164–2171. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
