

Spectrum of early lung cancer presentation in low-dose screening CT: a pictorial review
- PMID: 27188380
- PMCID: PMC4877352
- DOI: 10.1007/s13244-016-0487-4
Spectrum of early lung cancer presentation in low-dose screening CT: a pictorial review
Abstract
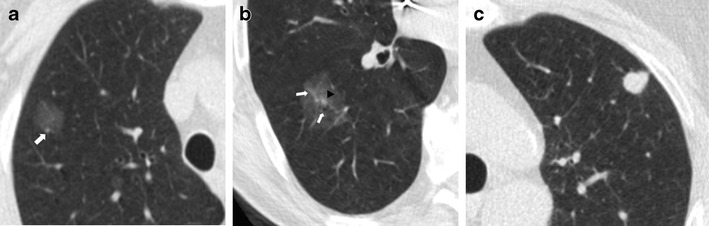
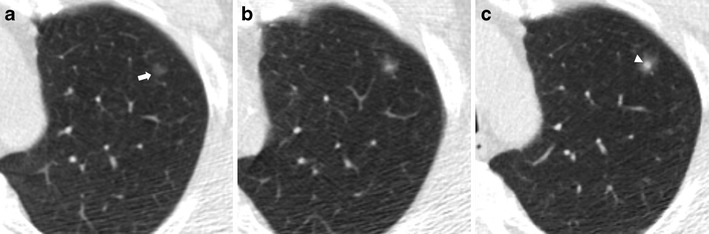
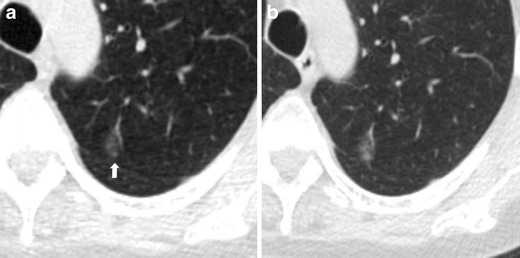
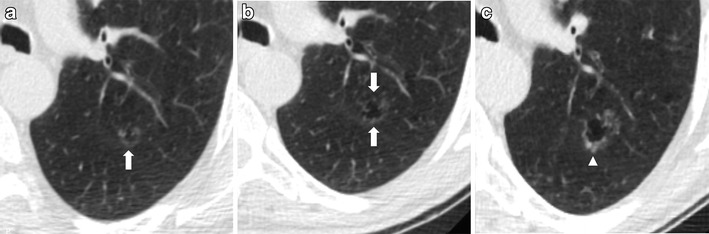
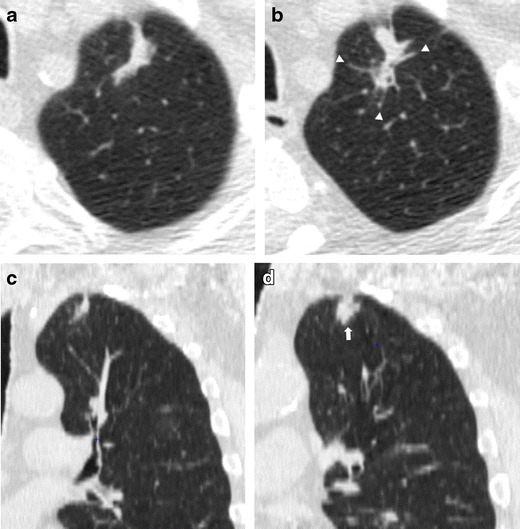
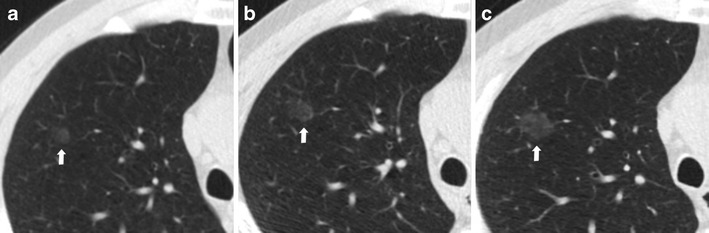
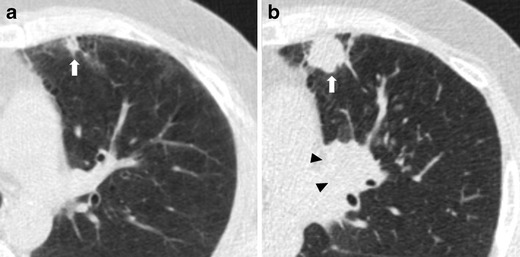
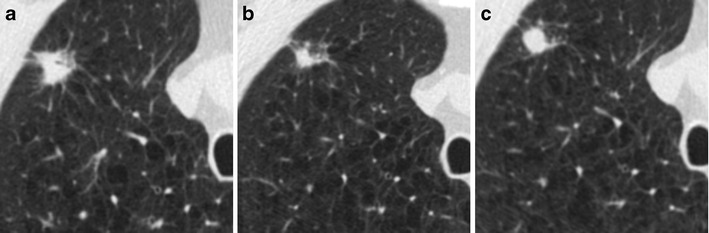
The typical presentation of early stage lung cancers on low-dose CT screening are non-calcified pulmonary nodules. However, there is a wide spectrum of unusual focal abnormalities that can be early presentations of lung cancer. These abnormalities include, for example, cancers associated with 'cystic airspaces' or scar-like cancers. The detection of lung cancer with low-dose CT can be affected by the absence of intravenous contrast medium. As a consequence, endobronchial and central lesions can be difficult to recognize, raising the potential for missed cancers. Focal lesions arising within pre-existing lung disease, such as lung fibrosis or apical scars, can also be early lung cancer manifestations and deserve particular consideration as recognition of these lesions may be hindered by the underlying disease. Furthermore, the unpredictable growth rate of lung cancer, which ranges from indolent to aggressive cancers, necessitates attention to the wide spectrum of progression in lung cancer appearance on serial low-dose CT scans. In this pictorial review we discuss the spectrum of early lung cancer presentation in low-dose CT screening, highlighting typical as well as unusual radiological features and the varied growth rates of early lung cancer. Teaching Points • There is a wide spectrum of early presentations of lung cancer on LDCT. • Low radiation dose and the absence of contrast medium injection can affect lung cancer detection. • Lung cancer growth shows various behaviours, ranging from indolent to aggressive cancers. • Familiarity with LDCT technique can improve CT screening effectiveness and avoid missed diagnosis.
Keywords: Low-dose CT; Lung cancer; Pulmonary nodule; Screening.
Figures
References
-
- Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, Fagerstrom RM, Gareen IF, Gatsonis C, Marcus PM, Sicks JD, National Lung Screening Trial Research Team Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395–409. doi: 10.1056/NEJMoa1102873. - DOI - PMC - PubMed
-
- Jaklitsch MT, Jacobson FL, Austin JH, Field JK, Jett JR, Keshavjee S, MacMahon H, Mulshine JL, Munden RF, Salgia R, Strauss GM, Swanson SJ, Travis WD, Sugarbaker DJ. The American Association for Thoracic Surgery guidelines for lung cancer screening using low-dose computed tomography scans for lung cancer survivors and other high-risk groups. J Thorac Cardiovasc Surg. 2012;144(1):33–38. doi: 10.1016/j.jtcvs.2012.05.060. - DOI - PubMed
-
- Wender R, Fontham ET, Barrera E, Jr, Colditz GA, Church TR, Ettinger DS, Etzioni R, Flowers CR, Gazelle GS, Kelsey DK, LaMonte SJ, Michaelson JS, Oeffinger KC, Shih YC, Sullivan DC, Travis W, Walter L, Wolf AM, Brawley OW, Smith RA. American Cancer Society lung cancer screening guidelines. CA Cancer J Clin. 2013;63(2):107–117. doi: 10.3322/caac.21172. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
