

Deaths, late deaths, and role of infecting dose in Ebola virus disease in Sierra Leone: retrospective cohort study
- PMID: 27188404
- PMCID: PMC4870382
- DOI: 10.1136/bmj.i2403
Deaths, late deaths, and role of infecting dose in Ebola virus disease in Sierra Leone: retrospective cohort study
Abstract
Objectives: To assess the frequency of fatal recrudescence from Ebola virus disease after discharge from treatment centres, and explore the influence of infecting dose on case fatality rates.
Design: Retrospective cohort study.
Setting: Western Area, Sierra Leone.
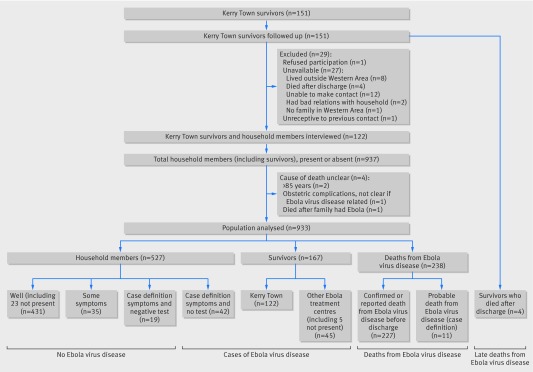
Participants: 151 survivors treated for Ebola virus disease at the Kerry Town treatment centre and discharged. Survivors were followed up for a vital status check at four to nine months after discharge, and again at six to 13 months after discharge. Verbal autopsies were conducted for four survivors who had died since discharge (that is, late deaths). Survivors still living in Western Area were interviewed together with their household members. Exposure level to Ebola virus disease was ascertained as a proxy of infecting dose, including for those who died.
Main outcome measures: Risks and causes of late death; case fatality rates; odds ratios of death from Ebola virus disease by age, sex, exposure level, date, occupation, and household risk factors.
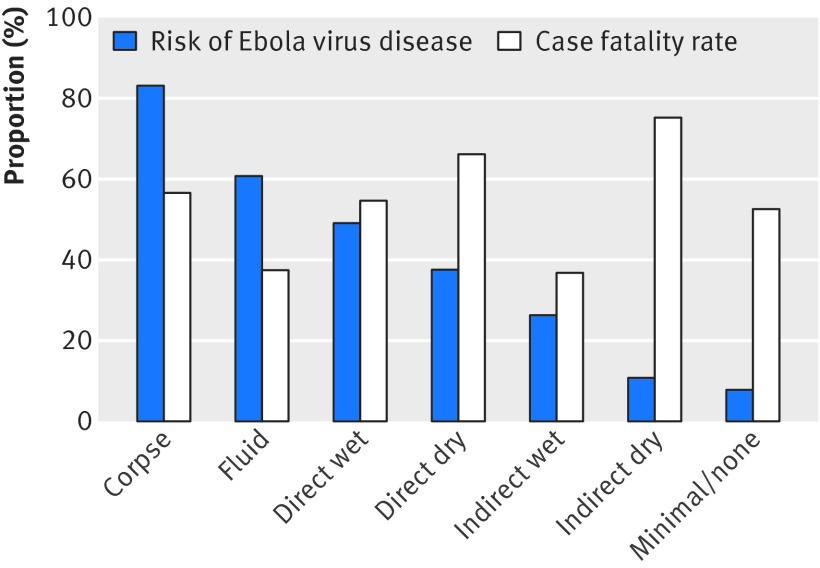
Results: Follow-up information was obtained on all 151 survivors of Ebola virus disease, a mean of 10 months after discharge. Four deaths occurred after discharge, all within six weeks: two probably due to late complications, one to prior tuberculosis, and only one after apparent full recovery, giving a maximum estimate of recrudescence leading to death of 0.7%. In these households, 395 people were reported to have had Ebola virus disease, of whom 227 died. A further 53 people fulfilled the case definition for probable disease, of whom 11 died. Therefore, the case fatality rate was 57.5% (227/395) for reported Ebola virus disease, or 53.1% (238/448) including probable disease. Case fatality rates were higher in children aged under 2 years and adults older than 30 years, in larger households, and in infections occurring earlier in the epidemic in Sierra Leone. There was no consistent trend of case fatality rate with exposure level, although increasing exposure increased the risk of Ebola virus disease.
Conclusions: In this study of survivors in Western Area, Sierra Leone, late recrudescence of severe Ebola virus disease appears to be rare. There was no evidence for an effect of infecting dose (as measured by exposure level) on the severity of disease.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

References
-
- Lefebvre A, Fiet C, Belpois-Duchamp C, Tiv M, Astruc K, Aho Glélé LS. Case fatality rates of Ebola virus diseases: a meta-analysis of World Health Organization data. Med Mal Infect 2014;44:412-6. 10.1016/j.medmal.2014.08.005 pmid:25193630. - DOI - PubMed
-
- Rosello A, Mossoko M, Flasche S, et al. Ebola virus disease in the Democratic Republic of the Congo, 1976-2014. Elife 2015;4:e09015 10.7554/eLife.09015 pmid:26525597. - DOI - PMC - PubMed
-
- Van Kerkhove MD, Bento AI, Mills HL, Ferguson NM, Donnelly CA. A review of epidemiological parameters from Ebola outbreaks to inform early public health decision-making. Sci Data 2015;2:150019 10.1038/sdata.2015.19 pmid:26029377. - DOI - PMC - PubMed
-
- WHO Ebola Response Team. Ebola virus disease among male and female persons in West Africa. N Engl J Med 2016;374:96-8. 10.1056/NEJMc1510305 pmid:26736011. - DOI - PMC - PubMed
-
- Ansumana R, Jacobsen KH, Sahr F, et al. Ebola in Freetown area, Sierra Leone—a case study of 581 patients. N Engl J Med 2015;372:587-8. 10.1056/NEJMc1413685 pmid:25539447. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical