

Varicella zoster virus infection
- PMID: 27188665
- PMCID: PMC5381807
- DOI: 10.1038/nrdp.2015.16
Varicella zoster virus infection
Abstract
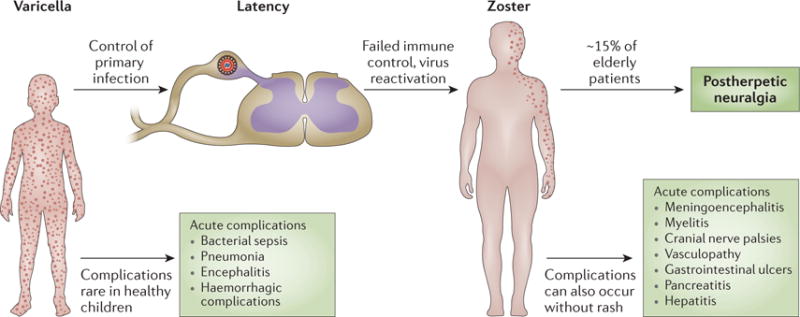
Infection with varicella zoster virus (VZV) causes varicella (chickenpox), which can be severe in immunocompromised individuals, infants and adults. Primary infection is followed by latency in ganglionic neurons. During this period, no virus particles are produced and no obvious neuronal damage occurs. Reactivation of the virus leads to virus replication, which causes zoster (shingles) in tissues innervated by the involved neurons, inflammation and cell death - a process that can lead to persistent radicular pain (postherpetic neuralgia). The pathogenesis of postherpetic neuralgia is unknown and it is difficult to treat. Furthermore, other zoster complications can develop, including myelitis, cranial nerve palsies, meningitis, stroke (vasculopathy), retinitis, and gastroenterological infections such as ulcers, pancreatitis and hepatitis. VZV is the only human herpesvirus for which highly effective vaccines are available. After varicella or vaccination, both wild-type and vaccine-type VZV establish latency, and long-term immunity to varicella develops. However, immunity does not protect against reactivation. Thus, two vaccines are used: one to prevent varicella and one to prevent zoster. In this Primer we discuss the pathogenesis, diagnosis, treatment, and prevention of VZV infections, with an emphasis on the molecular events that regulate these diseases. For an illustrated summary of this Primer, visit: http://go.nature.com/14xVI1.
Conflict of interest statement
J.B., J.I.C., R.J.C., M.D.G., D.G., C.G., S.H., M.N.O. and J.F.S. declare no competing interests. A.A.G. declares service contracts from Merck to investigate the safety of VZV vaccines (identifying VZV in samples from patients with possible adverse reactions), chairs an independent data monitoring committee for GlaxoSmithKline’s Phase III subunit glycoprotein E zoster vaccine trial, consults with Pfizer when invited, and has participated in an educational programme (supported by an unrestricted educational grant) on zoster for GlaxoSmithKline. P.G.E.K. has served on a scientific advisory board on zoster vaccination for Sanofi Pasteur MSD. Y.K. is Director General of the BIKEN foundation (The Research Foundation for Microbial Diseases of Osaka University), which produces varicella vaccines.
Figures

References
-
- Gershon AA, Takahashi M, Seward JF. In: Vaccines. Plotkin S, Orenstein W, Offit P, editors. Saunders Elsevier; 2011. pp. 915–958.
-
- Tsolia M, Gershon AA, Steinberg SP, Gelb L. Live attenuated varicella vaccine: evidence that the virus is attenuated and the importance of skin lesions in transmission of varicella-zoster virus. National Institute of Allergy and Infectious Diseases Varicella Vaccine Collaborative Study Group. J Pediatr. 1990;116:184–189. A study demonstrating that VZV spreads from skin lesions. - PubMed
-
- Chen JJ, Zhu Z, Gershon AA, Gershon MD. Mannose 6-phosphate receptor dependence of varicella zoster virus infection in vitro and in the epidermis during varicella and zoster. Cell. 2004;119:915–926. This study demonstrates the importance of the skin in VZV infection and identifies the cellular receptor that the virus uses for infection. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
