

Acute rheumatic fever and rheumatic heart disease
- PMID: 27188830
- PMCID: PMC5810582
- DOI: 10.1038/nrdp.2015.84
Acute rheumatic fever and rheumatic heart disease
Abstract
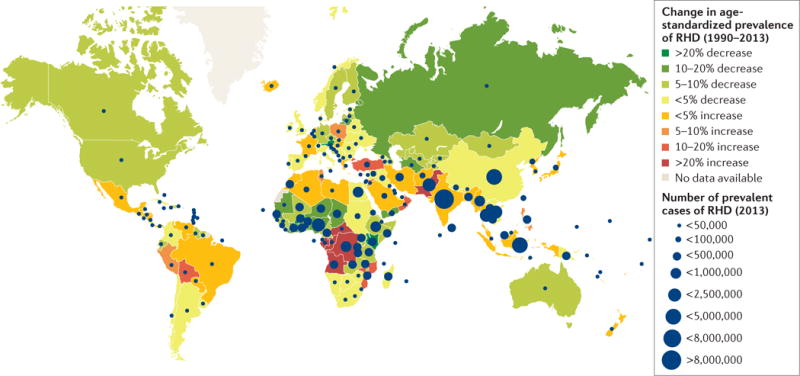
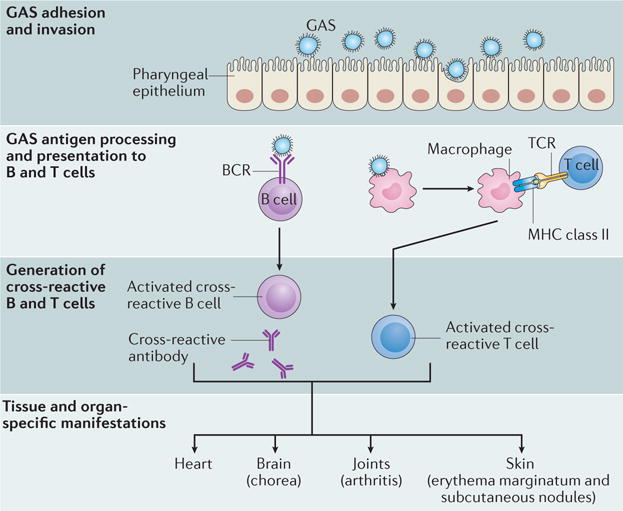
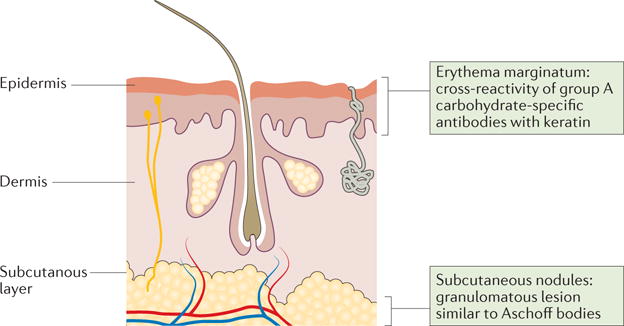
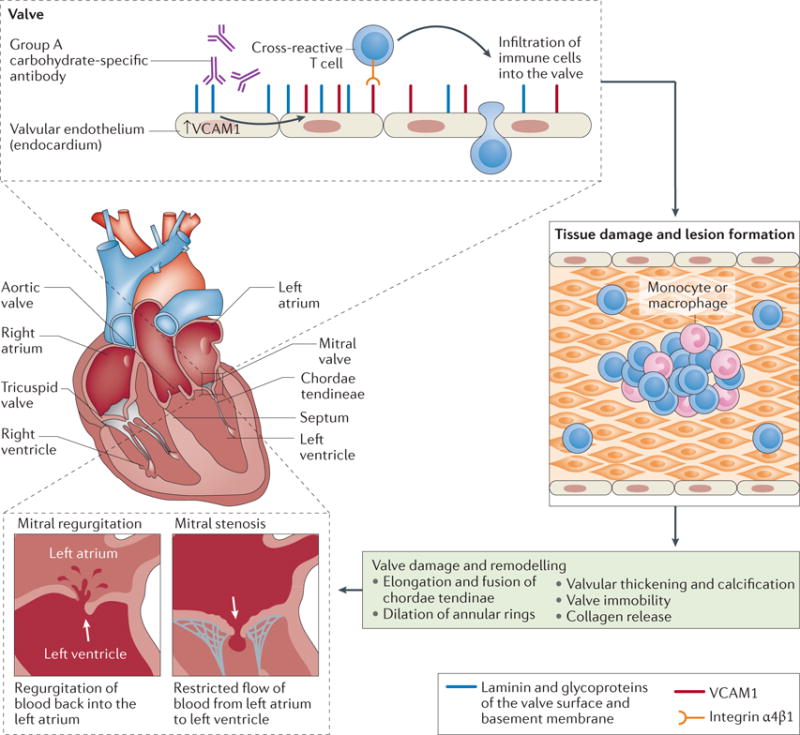
Acute rheumatic fever (ARF) is the result of an autoimmune response to pharyngitis caused by infection with group A Streptococcus. The long-term damage to cardiac valves caused by ARF, which can result from a single severe episode or from multiple recurrent episodes of the illness, is known as rheumatic heart disease (RHD) and is a notable cause of morbidity and mortality in resource-poor settings around the world. Although our understanding of disease pathogenesis has advanced in recent years, this has not led to dramatic improvements in diagnostic approaches, which are still reliant on clinical features using the Jones Criteria, or treatment practices. Indeed, penicillin has been the mainstay of treatment for decades and there is no other treatment that has been proven to alter the likelihood or the severity of RHD after an episode of ARF. Recent advances - including the use of echocardiographic diagnosis in those with ARF and in screening for early detection of RHD, progress in developing group A streptococcal vaccines and an increased focus on the lived experience of those with RHD and the need to improve quality of life - give cause for optimism that progress will be made in coming years against this neglected disease that affects populations around the world, but is a particular issue for those living in poverty.
Conflict of interest statement
G.K., L.Z., A.S., J.R.C., A.B., N.W., L.G., C.S., R.W. and B.M.M. have no conflict of interest. M.W.C. has financial interest in and is Chief Scientific Officer of Moleculera Labs, a company offering diagnostic testing for neurological disorders.
Figures
References
-
- Gewitz MH, et al. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association. Circulation. 2015;131:1806–1818. The 2015 revision of the Jones Criteria provides, for the first time, differing criteria for low and high disease incidence settings. - PubMed
-
- Denny FW, Wannamaker LW, Brink WR, Rammelkamp CH, Jr, Custer E. A Prevention of rheumatic fever; treatment of the preceding streptococcic infection. J Am Med Assoc. 1950;143:151–153. - PubMed
-
- Stollerman GH, Rusoff JH, Hirschfeld I. Prophylaxis against group A streptococci in rheumatic fever; the use of single monthly injections of benzathine penicillin G. N Engl J Med. 1955;252:787–792. - PubMed
-
- Carapetis JR. The stark reality of rheumatic heart disease. Eur Heart J. 2015;36:1070–1073. - PubMed
-
- Quinn RW. Comprehensive review of morbidity and mortality trends for rheumatic fever, streptococcal disease, and scarlet fever: the decline of rheumatic fever. Rev Infect Dis. 1989;11:928–953. This paper describes the first attempt to quantify the global disease burden resulting from ARF. Although the estimates did not incorporate many data from developing countries, this paper set the scene for subsequent disease burden estimates. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
