

Diabetic kidney disease
- PMID: 27188921
- PMCID: PMC7724636
- DOI: 10.1038/nrdp.2015.18
Diabetic kidney disease
Abstract
The kidney is arguably the most important target of microvascular damage in diabetes. A substantial proportion of individuals with diabetes will develop kidney disease owing to their disease and/or other co-morbidity, including hypertension and ageing-related nephron loss. The presence and severity of chronic kidney disease (CKD) identify individuals who are at increased risk of adverse health outcomes and premature mortality. Consequently, preventing and managing CKD in patients with diabetes is now a key aim of their overall management. Intensive management of patients with diabetes includes controlling blood glucose levels and blood pressure as well as blockade of the renin-angiotensin-aldosterone system; these approaches will reduce the incidence of diabetic kidney disease and slow its progression. Indeed, the major decline in the incidence of diabetic kidney disease (DKD) over the past 30 years and improved patient prognosis are largely attributable to improved diabetes care. However, there remains an unmet need for innovative treatment strategies to prevent, arrest, treat and reverse DKD. In this Primer, we summarize what is now known about the molecular pathogenesis of CKD in patients with diabetes and the key pathways and targets implicated in its progression. In addition, we discuss the current evidence for the prevention and management of DKD as well as the many controversies. Finally, we explore the opportunities to develop new interventions through urgently needed investment in dedicated and focused research. For an illustrated summary of this Primer, visit: http://go.nature.com/NKHDzg.
Figures
References
-
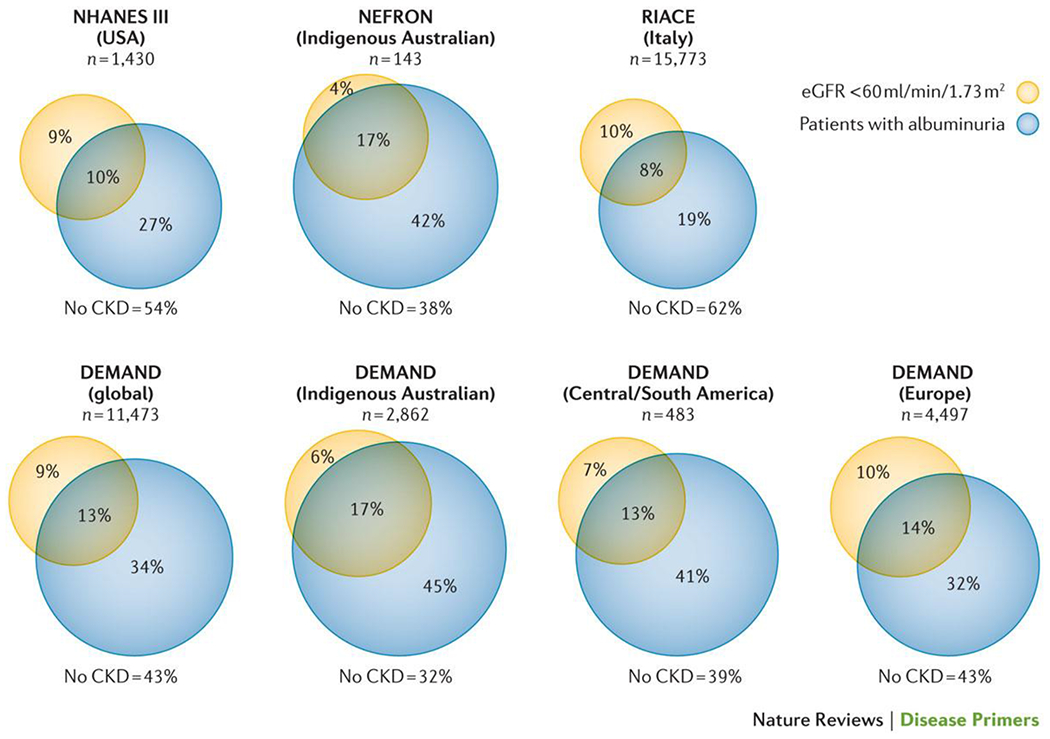
- Bruno G, et al. Estimated glomerular filtration rate, albuminuria and mortality in type 2 diabetes: the Casale Monferrato study. Diabetologia 50, 941–948 (2007). - PubMed
-
- Thomas MC, Weekes AJ, Broadley OJ, Cooper ME & Mathew TH The burden of chronic kidney disease in Australian patients with type 2 diabetes (the NEFRON study). The Medical journal of Australia 185, 140–144 (2006). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
