

Vascular Plug Assisted Retrograde Transvenous Obliteration (PARTO) for Gastric Varix Bleeding Patients in the Emergent Clinical Setting
- PMID: 27189294
- PMCID: PMC4951477
- DOI: 10.3349/ymj.2016.57.4.973
Vascular Plug Assisted Retrograde Transvenous Obliteration (PARTO) for Gastric Varix Bleeding Patients in the Emergent Clinical Setting
Abstract
Purpose: To evaluate the technical feasibility and safety of vascular plug assisted retrograde transvenous obliteration (PARTO) for bleeding gastric varix performed in the emergent clinical setting and describe the mid-term clinical results.
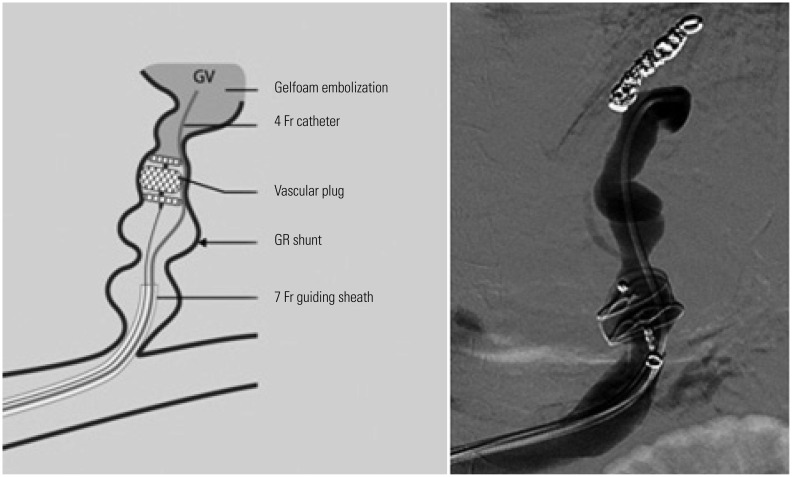
Materials and methods: From April 2012 to January 2015, emergent PARTO was tried in total 9 patients presented with active gastric varix bleeding. After initial insufficient or failure of endoscopic approach, they underwent PARTO in the emergent clinical setting. Gelatin sponge embolization of both gastrorenal (GR) shunt and gastric varix was performed after retrograde transvenous placement of a vascular plug in GR shunt. Coil assisted RTO (CARTO) was performed in one patient who had challenging GR shunt anatomy for vascular plug placement. Additional embolic materials, such as microcoils and NBCA glue-lipiodol mixture, were required in three patients to enhance complete occlusion of GR shunt or obliteration of competitive collateral vessels. Clinical success was defined as no variceal rebleeding and disappearance of gastric varix.
Results: All technical and clinical success-i.e., complete GR shunt occlusion and offending gastric varix embolization with immediate bleeding control-was achieved in all 9 patients. There was no procedure-related complication. All cases showed successful clinical outcome during mean follow up of 17 months (12-32 months), evidenced by imaging studies, endoscopy and clinical data. In 4 patients, mild worsening of esophageal varices or transient ascites was noted as portal hypertensive related change.
Conclusion: Emergent PARTO is technically feasible and safe, with acceptable mid-term clinical results, in treating active gastric varix bleeding.
Keywords: BRTO; Liver cirrhosis; PARTO; gastric varix; portal hypertension.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures


Similar articles
-
Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Variceal Hemorrhage.Korean J Radiol. 2016 Mar-Apr;17(2):230-8. doi: 10.3348/kjr.2016.17.2.230. Epub 2016 Mar 2. Korean J Radiol. 2016. PMID: 26957908 Free PMC article.
-
Comparison of Balloon-Occluded Retrograde Transvenous Obliteration (BRTO) Using Ethanolamine Oleate (EO), BRTO Using Sodium Tetradecyl Sulfate (STS) Foam and Vascular Plug-Assisted Retrograde Transvenous Obliteration (PARTO).Cardiovasc Intervent Radiol. 2016 Jun;39(6):840-6. doi: 10.1007/s00270-015-1288-8. Epub 2016 Jan 12. Cardiovasc Intervent Radiol. 2016. PMID: 26757912
-
Is salvage Plug-Assisted Retrograde Transvenous Obliteration (PARTO) safe and effective for bleeding gastric varices ?- A preliminary single-center experience.Emerg Radiol. 2024 Jun;31(3):359-365. doi: 10.1007/s10140-024-02232-2. Epub 2024 Apr 25. Emerg Radiol. 2024. PMID: 38664278
-
Modified Balloon-Occluded Retrograde Transvenous Obliteration (BRTO) Techniques for the Treatment of Gastric Varices: Vascular Plug-Assisted Retrograde Transvenous Obliteration (PARTO)/Coil-Assisted Retrograde Transvenous Obliteration (CARTO)/Balloon-Occluded Antegrade Transvenous Obliteration (BATO).Cardiovasc Intervent Radiol. 2018 Jun;41(6):835-847. doi: 10.1007/s00270-018-1896-1. Epub 2018 Feb 7. Cardiovasc Intervent Radiol. 2018. PMID: 29417267 Review.
-
Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Duodenal Variceal Bleeding - A Case Report and Literature Review.Korean J Gastroenterol. 2023 Dec 25;82(6):295-299. doi: 10.4166/kjg.2023.105. Korean J Gastroenterol. 2023. PMID: 38129999 Review.
Cited by
-
Evolution of Retrograde Transvenous Obliteration Techniques.Semin Intervent Radiol. 2018 Aug;35(3):185-193. doi: 10.1055/s-0038-1660796. Epub 2018 Aug 6. Semin Intervent Radiol. 2018. PMID: 30087521 Free PMC article. Review.
-
Endoscopic variceal obturation and retrograde transvenous obliteration for acute gastric cardiofundal variceal bleeding in liver cirrhosis.BMC Gastroenterol. 2022 Jul 26;22(1):355. doi: 10.1186/s12876-022-02428-1. BMC Gastroenterol. 2022. PMID: 35883035 Free PMC article.
-
Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Varices: The Role of Intra-Procedural Cone-Beam Computed Tomography.Korean J Radiol. 2018 Mar-Apr;19(2):223-229. doi: 10.3348/kjr.2018.19.2.223. Epub 2018 Feb 22. Korean J Radiol. 2018. PMID: 29520179 Free PMC article.
-
A comprehensive review of transvenous obliteration techniques in the management of gastric varices.Diagn Interv Radiol. 2023 Jan 31;29(1):146-154. doi: 10.5152/dir.2022.21193. Epub 2023 Jan 11. Diagn Interv Radiol. 2023. PMID: 36960571 Free PMC article. Review.
-
Assessment of hemodynamic changes in gastric varices using CT findings before and after vascular plug-assisted retrograde transvenous obliteration (PARTO) and evaluation of treatment outcomes.Abdom Radiol (NY). 2025 Jul;50(7):3148-3158. doi: 10.1007/s00261-024-04777-9. Epub 2024 Dec 21. Abdom Radiol (NY). 2025. PMID: 39707030
References
-
- de Franchis R, Primignani M. Natural history of portal hypertension in patients with cirrhosis. Clin Liver Dis. 2001;5:645–663. - PubMed
-
- Chang CJ, Hou MC, Liao WC, Chen PH, Lin HC, Lee FY, et al. Management of acute gastric varices bleeding. J Chin Med Assoc. 2013;76:539–546. - PubMed
-
- de Franchis R. Acute variceal haemorrhage: practice guidelines and real-life management. Dig Liver Dis. 2014;46:398–399. - PubMed
-
- Ryan BM, Stockbrugger RW, Ryan JM. A pathophysiologic, gastroenterologic, and radiologic approach to the management of gastric varices. Gastroenterology. 2004;126:1175–1189. - PubMed
-
- Kiyosue H, Ibukuro K, Maruno M, Tanoue S, Hongo N, Mori H. Multidetector CT anatomy of drainage routes of gastric varices: a pictorial review. Radiographics. 2013;33:87–100. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
